

When it is not primary progressive aphasia: A scoping review of spoken language impairment in other neurodegenerative dementias
- PMID: 34485677
- PMCID: PMC8409087
- DOI: 10.1002/trc2.12205
When it is not primary progressive aphasia: A scoping review of spoken language impairment in other neurodegenerative dementias
Abstract
Background: Progressive difficulties with spoken language occur across the spectrum of degenerative dementia. When not a primary presenting and dominant symptom, language difficulties may be overlooked in favor of more prominent cognitive, behavior, or motor deficits. The aim of this scoping review is to examine the extent and nature of the research evidence describing (1) the spoken language impairments found in non-language led dementias, (2) their impact on everyday living, and (3) the reported language interventions.
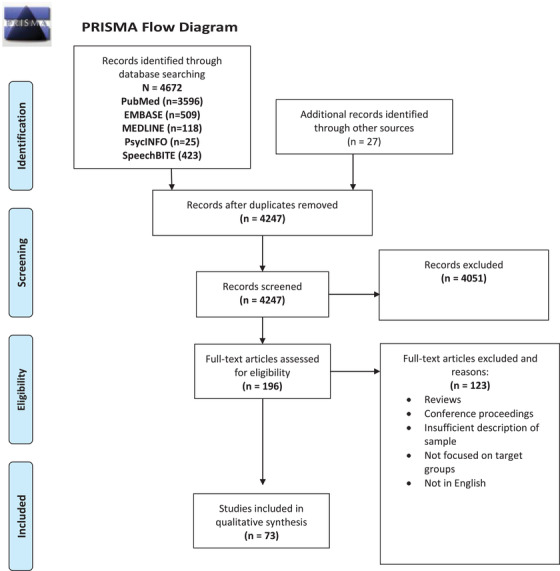
Methods: We searched PubMed, MEDLINE, OVID-EMBASE, PsycINFO, and SpeechBITE using terms related to spoken language for the following dementia types: Parkinson's disease dementia (PDD), dementia with Lewy bodies (DLB), progressive supranuclear palsy (PSP), cortico-basal syndrome (CBS), behavior variant frontotemporal dementia (bvFTD), early-onset Alzheimer's disease (EOAD), posterior cortical atrophy (PCA), and motor neuron disease associated with FTD (MND+FTD). Risk of bias was assessed with the QualSyst tool.
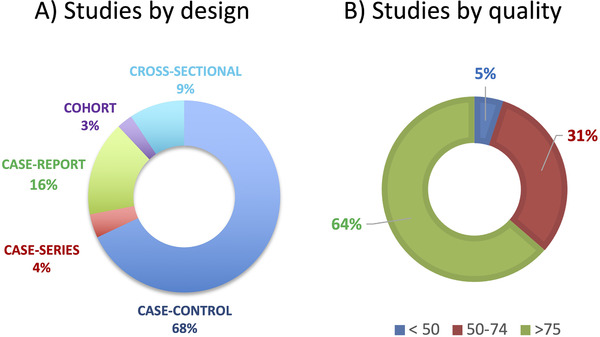
Results: Seventy-three eligible studies were included. A wide range of spoken language impairments were reported, involving both linguistic (e.g., syntactic processing) and other cognitive (e.g., sustained attention) underlying mechanisms. Although the severity of these deficits was scarcely reported, in some cases they manifested as non-fluent, dynamic, and global aphasias. No papers in the review described either the impact of these language impairments on everyday living or language therapies to treat them.
Discussion: There is a need to understand better the level of disability produced by language impairment in people living with non-language-led dementias. Our findings suggest three calls for action: (1) research studies should assess the clinical relevance of any spoken language deficits examined, (2) both linguistic and cognitive underlying mechanisms should be fully described (to inform the design of effective language and behavioral interventions), and (3) trials of language therapy should be conducted in those groups of individuals where significant language impairment is proved.
Keywords: aphasia; communication disorders; dementia; language therapy; spoken language.
© 2021 The Authors. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring published by Wiley Periodicals, LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Cotelli M, Mannenti R, Ferrari C, Gobbi E, Macis A, Cappa SF. Effectiveness of language training and non‐invasive brain stimulation on oral and written naming performance in primary progressive aphasia: a meta‐analysis and systematic review. Neurosci Biobehav Rev. 2020(108):498‐525. - PubMed
-
- Imamura T, Takatsuki Y, Fujimori M, et al. Age at onset and language disturbances in Alzheimer's disease. Neuropsychologia. 1998;36(9):945‐949. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous