

Antimicrobial resistance in paediatric Streptococcus pneumoniae isolates amid global implementation of pneumococcal conjugate vaccines: a systematic review and meta-regression analysis
- PMID: 34485957
- PMCID: PMC8410609
- DOI: 10.1016/S2666-5247(21)00064-1
Antimicrobial resistance in paediatric Streptococcus pneumoniae isolates amid global implementation of pneumococcal conjugate vaccines: a systematic review and meta-regression analysis
Abstract
Background: Pneumococcal diseases are a leading cause of morbidity and mortality among children globally, and the burden of these diseases might be worsened by antimicrobial resistance. To understand the effect of pneumococcal conjugate vaccine (PCV) deployment on antimicrobial resistance in pneumococci, we assessed the susceptibility of paediatric pneumococcal isolates to various antimicrobial drugs before and after PCV implementation.
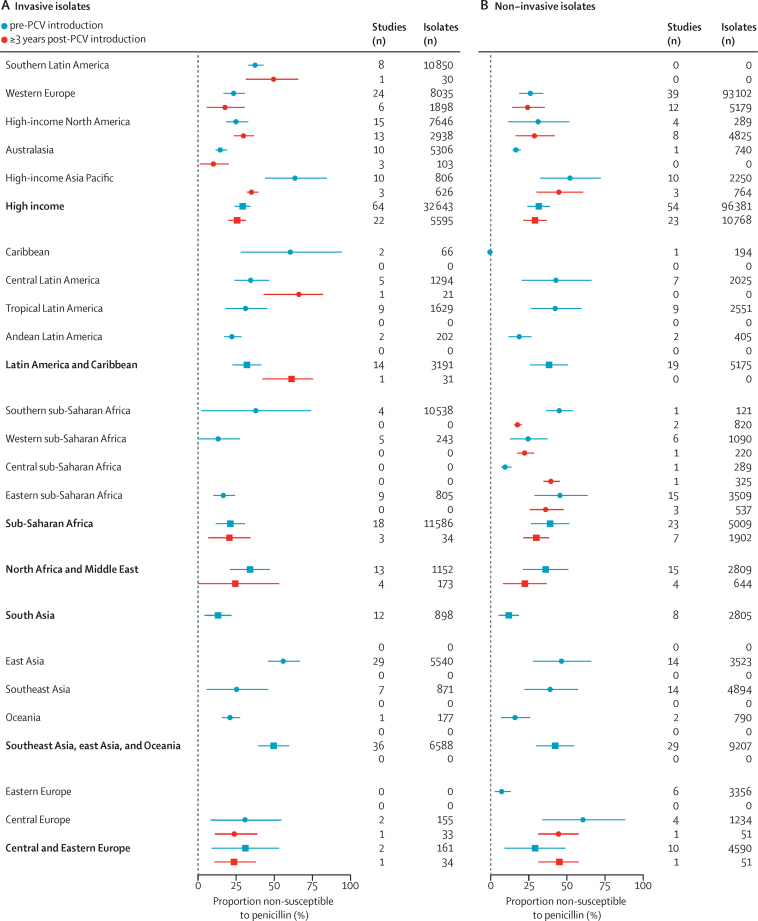
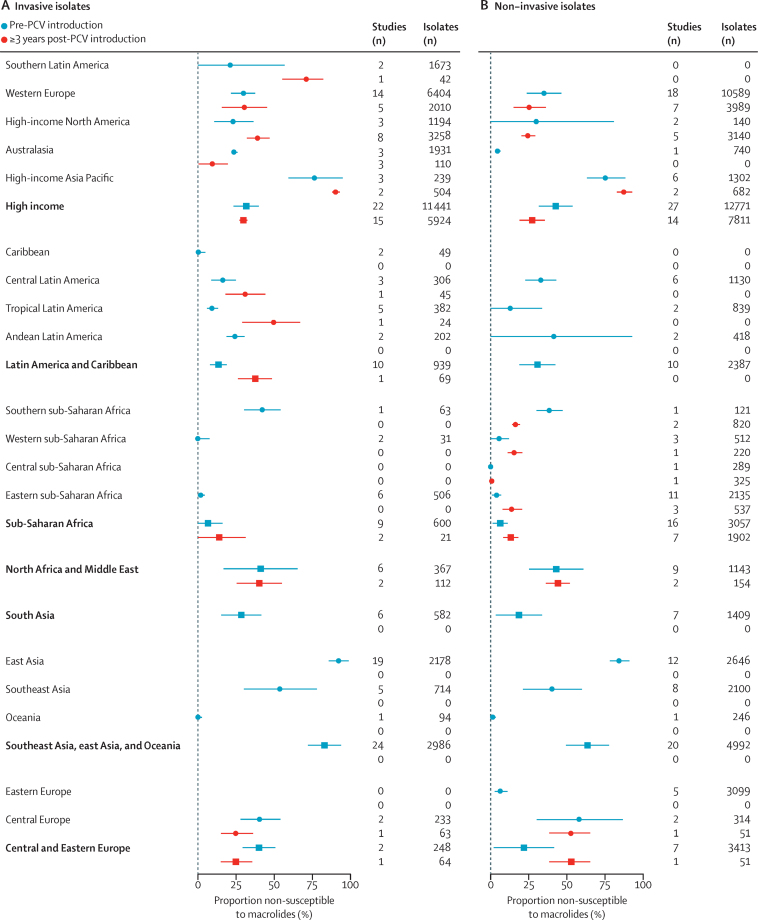
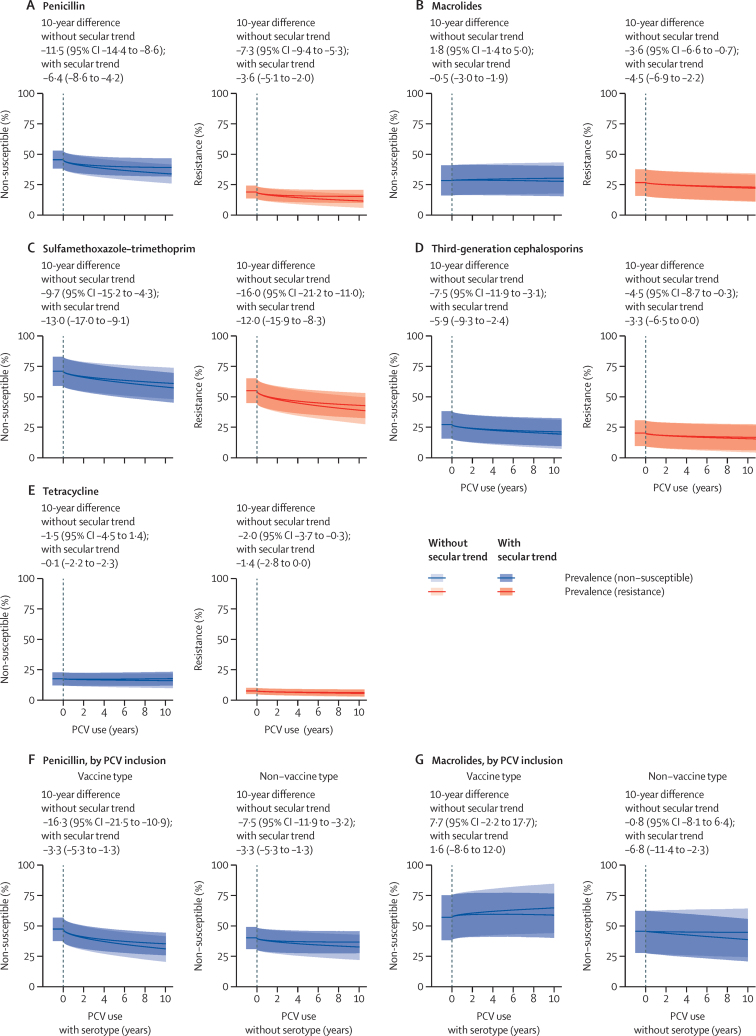
Methods: We did a systematic review of studies reporting antimicrobial susceptibility profiles of paediatric pneumococcal isolates between 2000 and 2020 using PubMed and the Antimicrobial Testing Leadership and Surveillance database (ATLAS; Pfizer). Population-based studies of invasive pneumococcal disease or nasopharyngeal colonisation were eligible for inclusion. As primary outcome measures, we extracted the proportions of isolates that were non-susceptible or resistant to penicillin, macrolides, sulfamethoxazole-trimethoprim, third-generation cephalosporins, and tetracycline from each study. Where available, we also extracted data on pneumococcal serotypes. We estimated changes in the proportion of isolates with reduced susceptibility or resistance to each antibiotic class using random-effects meta-regression models, adjusting for study-level and region-level heterogeneity, as well as secular trends, invasive or colonising isolate source, and countries' per-capita gross domestic product.
Findings: From 4910 studies screened for inclusion, we extracted data from 559 studies on 312 783 paediatric isolates. Susceptibility of isolates varied substantially across regions both before and after implementation of any PCV product. On average across all regions, we estimated significant absolute reductions in the proportions of pneumococci showing non-susceptibility to penicillin (11·5%, 95% CI 8·6-14·4), sulfamethoxazole-trimethoprim (9·7%, 4·3-15·2), and third-generation cephalosporins (7·5%, 3·1-11·9), over the 10 years after implementation of any PCV product, and absolute reductions in the proportions of pneumococci resistant to penicillin (7·3%, 5·3-9·4), sulfamethoxazole-trimethoprim (16·0%, 11·0-21·2), third-generation cephalosporins (4·5%, 0·3-8·7), macrolides (3·6%, 0·7-6·6) and tetracycline (2·0%, 0·3-3·7). We did not find evidence of changes in the proportion of isolates non-susceptible to macrolides or tetracycline after PCV implementation. Observed changes in penicillin non-susceptibility were driven, in part, by replacement of vaccine-targeted serotypes with non-vaccine serotypes that were less likely to be non-susceptible.
Interpretation: Implementation of PCVs has reduced the proportion of circulating pneumococci resistant to first-line antibiotic treatments for pneumonia. This effect merits consideration in assessments of vaccine impact and investments in coverage improvements.
Funding: Bill & Melinda Gates Foundation.
© 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Conflict of interest statement
JAL has received grants and consulting fees from Pfizer and Merck Sharp & Dohme; and consulting fees from VaxCyte and Kaiser Permanente, unrelated to the submitted work. All other authors declare no competing interests.
Figures
References
-
- Bogaert D, De Groot R, Hermans PWM. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis. 2004;4:144–154. - PubMed
-
- Buckley BS, Henschke N, Bergman H. Impact of vaccination on antibiotic usage: a systematic review and meta-analysis. Clin Microbiol Infect. 2019;25:1213–1225. - PubMed
-
- Evans W, Hansman D. Tetracycline-resistant pneumococcus. Lancet. 1963;281:451. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
