

Severity of Severe Acute Respiratory System Coronavirus 2 (SARS-CoV-2) Alpha Variant (B.1.1.7) in England
- PMID: 34487522
- PMCID: PMC8522415
- DOI: 10.1093/cid/ciab754
Severity of Severe Acute Respiratory System Coronavirus 2 (SARS-CoV-2) Alpha Variant (B.1.1.7) in England
Abstract
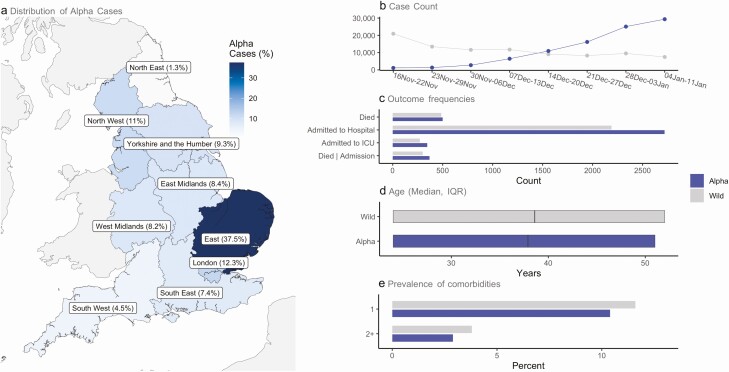
Background: The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) alpha variant (B.1.1.7) is associated with higher transmissibility than wild-type virus, becoming the dominant variant in England by January 2021. We aimed to describe the severity of the alpha variant in terms of the pathway of disease from testing positive to hospital admission and death.
Methods: With the approval of NHS England, we linked individual-level data from primary care with SARS-CoV-2 community testing, hospital admission, and Office for National Statistics all-cause death data. We used testing data with S-gene target failure as a proxy for distinguishing alpha and wild-type cases, and stratified Cox proportional hazards regression to compare the relative severity of alpha cases with wild-type diagnosed from 16 November 2020 to 11 January 2021.
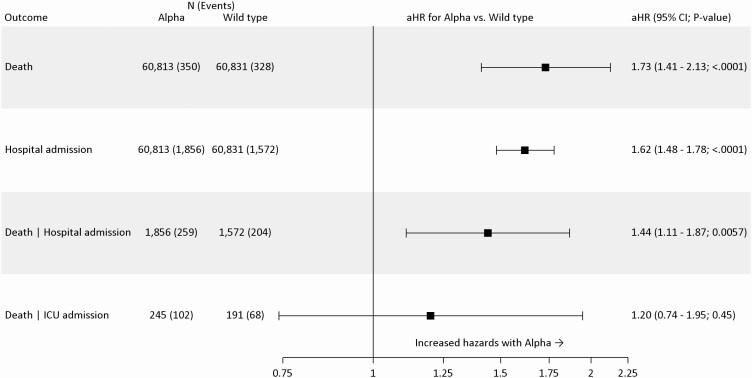
Results: Using data from 185 234 people who tested positive for SARS-CoV-2 in the community (alpha = 93 153; wild-type = 92 081), in fully adjusted analysis accounting for individual-level demographics and comorbidities as well as regional variation in infection incidence, we found alpha associated with 73% higher hazards of all-cause death (adjusted hazard ratio [aHR]: 1.73; 95% confidence interval [CI]: 1.41-2.13; P < .0001) and 62% higher hazards of hospital admission (1.62; 1.48-1.78; P < .0001) compared with wild-type virus. Among patients already admitted to the intensive care unit, the association between alpha and increased all-cause mortality was smaller and the CI included the null (aHR: 1.20; 95% CI: .74-1.95; P = .45).
Conclusions: The SARS-CoV-2 alpha variant is associated with an increased risk of both hospitalization and mortality than wild-type virus.
Keywords: SARS-CoV-2; alpha; case fatality; hospital admission.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Public Health England. Investigation of novel SARS-CoV-2 variant: variant of concern 202012/01. Technical briefing document on novel SARS-CoV-2 variant. Available at: https://www.gov.uk/government/publications/investigation-of-novel-sars-c.... Accessed 25 February 2021.
-
- Public Health England. Investigation of SARS-CoV-2 variants of concern in England: technical briefing 6.2021. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploa.... Accessed 7 March 2021.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
