

Thinking inside the box: Current insights into targeting orbital tissue remodeling and inflammation in thyroid eye disease
- PMID: 34487739
- PMCID: PMC8891393
- DOI: 10.1016/j.survophthal.2021.08.010
Thinking inside the box: Current insights into targeting orbital tissue remodeling and inflammation in thyroid eye disease
Abstract
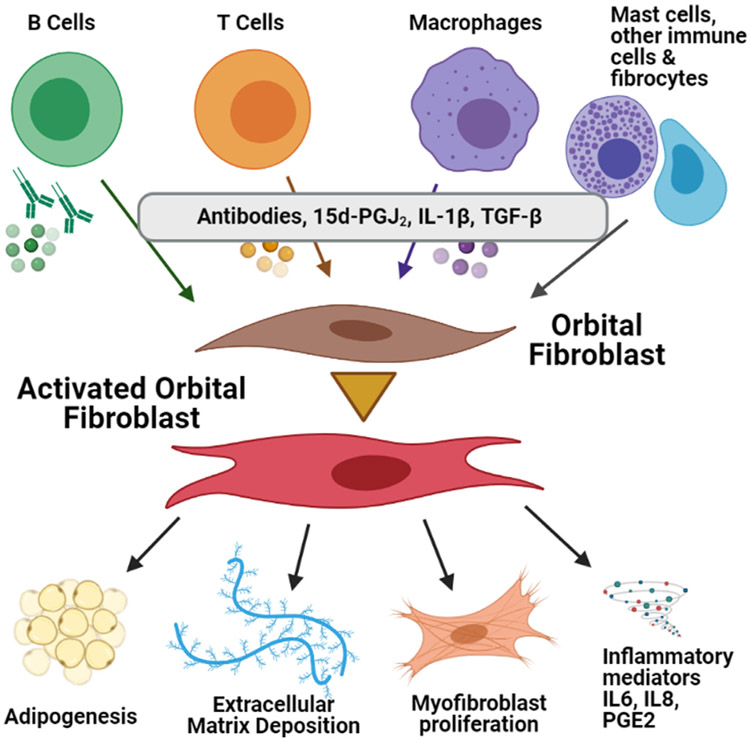
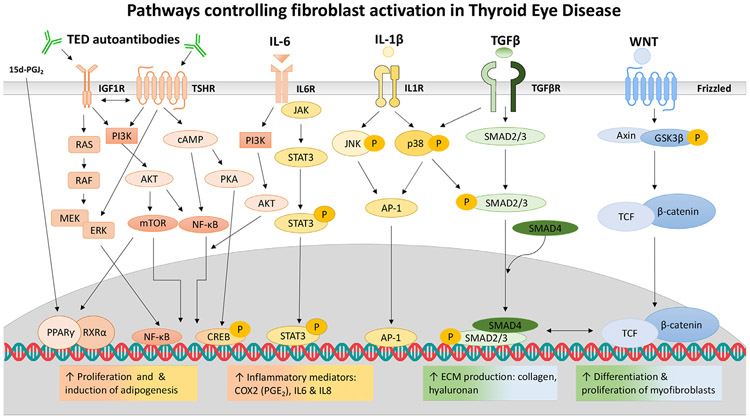
Thyroid eye disease (TED) is an autoimmune disorder that manifests in the orbit. In TED, the connective tissue behind the eye becomes inflamed and remodels with increased fat accumulation and/or increased muscle and scar tissue. As orbital tissue expands, patients develop edema, exophthalmos, diplopia, and optic neuropathy. In severe cases vision loss may occur secondary to corneal scarring from exposure or optic nerve compression. Currently there is no cure for TED, and treatments are limited. A major breakthrough in TED therapy occurred with the FDA approval of teprotumumab, a monoclonal insulin-like growth factor 1 receptor (IGF1R) blocking antibody. Yet, teprotumumab therapy has limitations, including cost, infusion method of drug delivery, variable response, and relapse. We describe approaches to target orbital fibroblasts and the complex pathophysiology that underlies tissue remodeling and inflammation driving TED. Further advances in the elucidation of the mechanisms of TED may lead to prophylaxis based upon early biomarkers as well as lead to more convenient, less expensive therapies.
Keywords: Graves’ orbitopathy; Thyroid eye disease; fibroblast; insulin-like growth factor 1 receptor; microRNA; orbital fibroblast; teprotumumab; therapeutics, targeted therapy.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest
No conflicting relationship exist for any author.
Figures

References
-
- Adamidou F, Anagnostis P, Boboridis K, Manani C, Georgiou T, Veneti S, et al. Enduring remission of active and sight-threatening Graves’ orbitopathy with rituximab: report of two cases. Endocr J. 2018;65(9):963–7. - PubMed
-
- Alevizaki M, Mantzou E, Cimponeriu A, Saltiki K, Philippou G, Wiersinga W. The Pro 12 Ala PPAR gamma gene polymorphism: possible modifier of the activity and severity of thyroid-associated orbitopathy (TAO). Clin Endocrinol (Oxf). 2009;70(3):464–8. - PubMed
-
- Allen RC, Bradley EA, Fante RG, Lucarelli MJ. A perspective on the current role of teprotumumab in treatment of thyroid eye disease. Ophthalmology. 2021;128(8):1125–8. - PubMed
-
- Ameres SL, Zamore PD. Diversifying microRNA sequence and function. Nat Rev Mol Cell Biol. 2013;14(8):475–88. - PubMed
-
- Antoszczak M, Huczynski A. Salinomycin and its derivatives - A new class of multiple-targeted "magic bullets". Eur J Med Chem. 2019;176:208–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
