

Association between serum phosphate and mortality in critically ill patients: a large retrospective cohort study
- PMID: 34489265
- PMCID: PMC8422318
- DOI: 10.1136/bmjopen-2020-044473
Association between serum phosphate and mortality in critically ill patients: a large retrospective cohort study
Abstract
Objectives: This research aims to explore the impact of serum phosphate on the mortality of critically ill patients.
Design: A retrospective large cohort study.
Setting: Our data were extracted from a publicly accessible database named 'Multiparameter Intelligent Monitoring in Intensive Care Database III'.
Participants: 27 131 patients were included by clear definitions of selection and exclusion criteria.
Interventions: We used initial phosphate at admission as a design variable. Patients were divided into six groups with different serum phosphate levels and five groups at different intensive care unit (ICU) departments.
Primary and secondary outcomes: 28-day and 90-day mortality were primary outcomes. All-cause mortality and length of stay ICU were secondary outcomes.
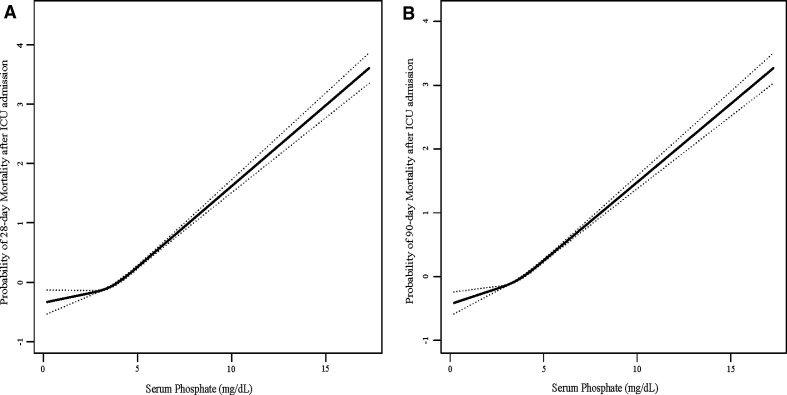
Results: Patients with very-high-normal serum phosphate, hypophosphataemia and hyperphosphataemia had worse outcomes. And the relationship between serum phosphate and the probability of 28-day or 90-day mortality had a linear relationship. After adjustment for potential confounders, hypophosphataemia and hyperphosphataemia were not significantly associated with 28-day or 90-day mortality. Nevertheless, at the medical ICU, hyperphosphataemia was associated with increased 28-day or 90-day mortality (HR=0.64, 95% CI 0.48 to 0.84, p=0.0017; HR=0.72, 95% CI 0.57 to 0.91, p=0.0067, respectively), using group 2 (≥2.5 mg/dL and <3.0 mg/dL) as the reference group.
Conclusions: Patients with very-high-normal serum phosphate also had worse outcomes, it might be necessary to re-evaluate the definitions of the normal reference range for serum phosphate. Hypophosphataemia and hyperphosphataemia are not the independent risk factors of 28-day or 90-day ICU mortality, which leads us to consider whether phosphate monitoring is not a necessary measure in critically ill patients. But hyperphosphataemia was associated with increased 28-day or 90-day mortality at the medical ICU, which emphasises the potential importance of early diagnosis and treatment of hyperphosphataemia for the patients who were admitted to the medical ICU.
Keywords: adult intensive & critical care; human resource management; intensive & critical care.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Phosphate abnormalities and outcomes among admissions to the intensive care unit: A retrospective multicentre cohort study.J Crit Care. 2021 Aug;64:154-159. doi: 10.1016/j.jcrc.2021.03.012. Epub 2021 Apr 18. J Crit Care. 2021. PMID: 33906104
-
Association Between Dexamethasone and Delirium in Critically Ill Patients: A Retrospective Cohort Study of a Large Clinical Database.J Surg Res. 2021 Jul;263:89-101. doi: 10.1016/j.jss.2021.01.027. Epub 2021 Feb 24. J Surg Res. 2021. PMID: 33639374
-
Moderate to severe hyperphosphataemia as an independent prognostic factor for 28-day mortality in adult patients with sepsis.Emerg Med J. 2020 Jun;37(6):355-361. doi: 10.1136/emermed-2019-208976. Epub 2020 Apr 22. Emerg Med J. 2020. PMID: 32321706
-
Association between early elevated phosphate and mortality among critically ill elderly patients: a retrospective cohort study.BMC Geriatr. 2022 Mar 15;22(1):208. doi: 10.1186/s12877-022-02920-z. BMC Geriatr. 2022. PMID: 35291970 Free PMC article.
-
Hypophosphataemia in Critical Illness: A Narrative Review.J Clin Med. 2024 Nov 26;13(23):7165. doi: 10.3390/jcm13237165. J Clin Med. 2024. PMID: 39685625 Free PMC article. Review.
Cited by
-
Association Between the Serum Phosphate Levels and Hospital Mortality as Well as 90-Day Mortality Among Critically Ill Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study.Int J Chron Obstruct Pulmon Dis. 2024 Jul 18;19:1681-1693. doi: 10.2147/COPD.S465752. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39055391 Free PMC article.
-
Hyperphosphatemia and Outcomes in Critically Ill Patients: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2022 May 17;9:870637. doi: 10.3389/fmed.2022.870637. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35665344 Free PMC article.
-
Elevated Initial Serum Phosphate Levels Predict Higher Mortality and Impaired Neurological Outcome in Cardiac Arrest Patients with Return of Spontaneous Circulation.Diagnostics (Basel). 2023 Jan 28;13(3):479. doi: 10.3390/diagnostics13030479. Diagnostics (Basel). 2023. PMID: 36766585 Free PMC article.
-
Relationship between serum phosphate and mortality in critically ill children receiving continuous renal replacement therapy.Front Pediatr. 2023 Apr 12;11:1129156. doi: 10.3389/fped.2023.1129156. eCollection 2023. Front Pediatr. 2023. PMID: 37124175 Free PMC article.
-
Association between serum phosphate and in-hospital mortality of patients with AECOPD: A retrospective analysis on eICU database.Heliyon. 2023 Sep 6;9(9):e19748. doi: 10.1016/j.heliyon.2023.e19748. eCollection 2023 Sep. Heliyon. 2023. PMID: 37809538 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources