

Relapse prevention group therapy via video-conferencing for substance use disorder: protocol for a multicentre randomised controlled trial in Indonesia
- PMID: 34489288
- PMCID: PMC8422497
- DOI: 10.1136/bmjopen-2021-050259
Relapse prevention group therapy via video-conferencing for substance use disorder: protocol for a multicentre randomised controlled trial in Indonesia
Abstract
Background: Substance use disorder (SUD) is a leading contributor to the global burden of disease. In Indonesia, the availability of formal treatment for SUD falls short of the targeted coverage. A standardised therapeutic option for SUD with potential for widespread implementation is required, yet evidence-based data in the country are scarce. In this study, we developed a cognitive behavioural therapy (CBT)-based group telemedicine model and will investigate effectiveness and implementability in a multicentre randomised controlled trial.
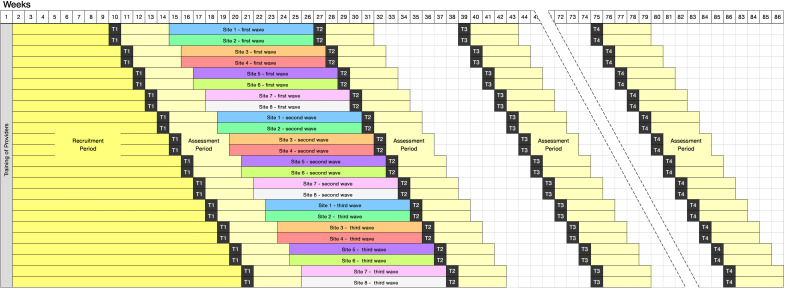
Methods: A total of 220 participants will be recruited from the social networks of eight sites in Indonesia: three hospitals, two primary healthcare centres and three rehabilitation centres. The intervention arm will participate in a relapse prevention programme called the Indonesia Drug Addiction Relapse Prevention Programme (Indo-DARPP), a newly developed 12-week module based on CBT and motivational interviewing constructed in the Indonesian context. The programme will be delivered by a healthcare provider and a peer counsellor in a group therapy setting via video-conferencing, as a supplement to participants' usual treatments. The control arm will continue treatment as usual. The primary outcome will be the percentage increase in days of abstinence from the primarily used substance in the past 28 days. Secondary outcomes will include addiction severity, quality of life, motivation to change, psychiatric symptoms, cognitive function, coping, and internalised stigma. Assessments will be performed at baseline (week 0), post-treatment (week 13), and 3 and 12 months post-treatment completion (weeks 24 and 60). Retention, participant satisfaction, and cost-effectiveness will be assessed as the implementation outcomes.
Ethics and dissemination: The study protocol was reviewed and approved by the Ethics Committees of Universitas Indonesia and Kyoto University. The results will be disseminated via academic journals and international conferences. Depending on trial outcomes, the treatment programme will be advocated for adoption as a formal healthcare-based approach for SUD.
Trial registration number: UMIN000042186.
Keywords: clinical trials; psychiatry; substance misuse; telemedicine.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- GBD 2016 Alcohol and Drug Use Collaborators . The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Psychiatry 2018;5:987–1012. 10.1016/S2215-0366(18)30337-7 - DOI - PMC - PubMed
-
- United Nations Office on Drugs and Crimes . World drug report 2020. Vienna: UNODC, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous