

Upper Extremity Deep Vein Thrombosis and Asymptomatic Vein Occlusion in Patients With Transvenous Leads: A Systematic Review and Meta-Analysis
- PMID: 34490367
- PMCID: PMC8416492
- DOI: 10.3389/fcvm.2021.698336
Upper Extremity Deep Vein Thrombosis and Asymptomatic Vein Occlusion in Patients With Transvenous Leads: A Systematic Review and Meta-Analysis
Abstract
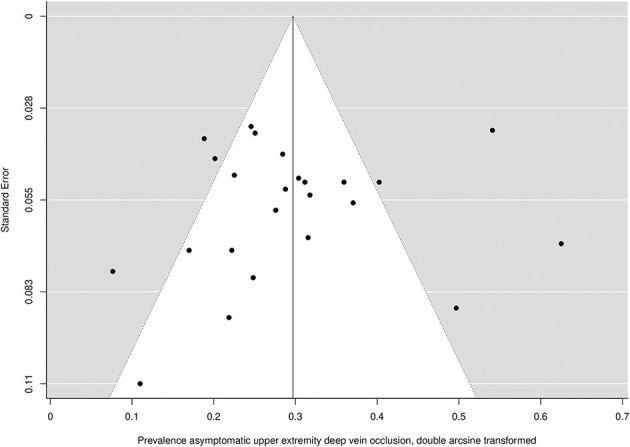
Aims: The presence of transvenous leads for cardiac device therapy may increase the risk of venous thromboembolisms. The epidemiology of these complications has not yet been determined systematically. Therefore, this study aims to determine (I) the incidence of symptomatic upper extremity deep vein thrombosis (UEDVT) and (II) the prevalence of asymptomatic upper extremity vein occlusion in patients with transvenous leads, both after the initial 2 months following lead implantation. Methods: PubMed, EMBASE, and Cochrane Library were searched until March 31, 2020 to identify studies reporting incidence of UEDVT and prevalence of asymptomatic vein occlusion after the initial 2 months after implantation in adult patients with transvenous leads. Incidence per 100 patient years of follow-up (PY) and proportions (%) were calculated to derive pooled estimates of incidence and prevalence. Results: Search and selection yielded 20 and 24 studies reporting on UEDVT and asymptomatic vein occlusion, respectively. The overall pooled incidence of UEDVT was 0.9 (95% CI 0.5-1.4) per 100PY after 2 months after lead implantation. High statistical heterogeneity was present among studies (I2 = 82.4%; P = < 0.001) and only three studies considered to be at low risk of bias. The overall pooled prevalence of asymptomatic upper extremity vein occlusion was 8.6% (95% CI 6.0-11.5) with high heterogeneity (I2 = 81.4%; P = <0.001). Meta-regression analysis showed more leads to be associated with a higher risk of UEDVT. Conclusion: Transvenous leads are an important risk factor for symptomatic UEDVT, which may occur up to multiple years after initial lead implantation. Existing data on UEDVT after lead implantation is mostly of poor quality, which emphasizes the need for high quality prospective research. Asymptomatic vein occlusion is present in a substantial proportion of patients and may complicate any future lead addition. Clinical Trial Registration: (URL: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020178136, Identifier: PROSPERO 2020 CRD42020178136).
Keywords: cardiac device therapy; deep vein thrombosis; epidemiology; systematic review and meta-analysis; transvenous leads.
Copyright © 2021 Duijzer, de Winter, Nijkeuter, Tuinenburg and Westerink.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Raatikainen MJP, Arnar DO, Zeppenfeld K, Merino JL, Levya F, Hindriks G, et al. . Statistics on the use of cardiac electronic devices and electrophysiological procedures in the European Society of Cardiology countries: 2014 report from the European Heart Rhythm Association. Europace. (2015) 17(Suppl. 1):i1–75. 10.1093/europace/euu300 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources