

Dermoscopic Evaluation of Inflammatory Nail Disorders and Their Mimics
- PMID: 34490472
- PMCID: PMC9425608
- DOI: 10.2340/00015555-3917
Dermoscopic Evaluation of Inflammatory Nail Disorders and Their Mimics
Abstract
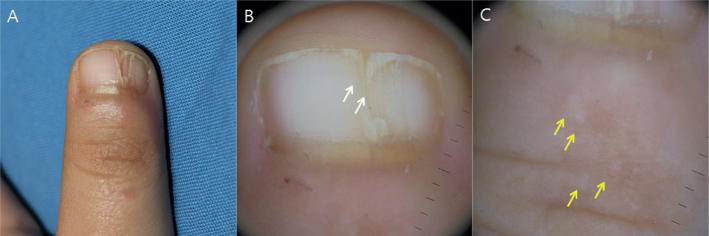
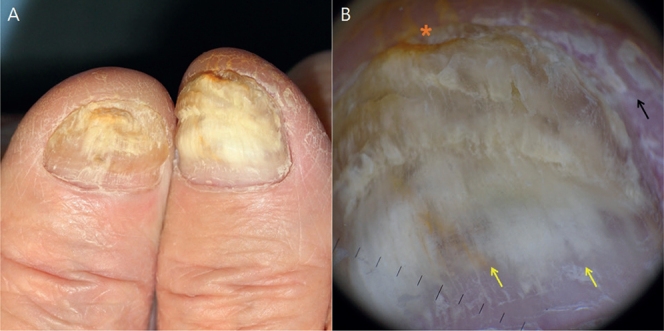
Nail dermoscopy (onychoscopy) is a valuable diagnostic tool for evaluating diseases in the nail apparatus. It is non-invasive, allowing clinicians to prioritize particular nails for biopsy. Thus, it can improve diagnostic accuracy and expedite treatment. Evaluating inflammatory nail disorders using onychoscopy is a relatively new approach to clinical assessment and has the potential to augment clinical care. This review highlights key dermoscopic features of major inflammatory nail disorders, including trachyonychia, nail psoriasis, nail lichen planus, onychotillomania, nail lichen striatus and allergic contact dermatitis due to artificial nails. It also illustrates their management and differential diagnoses, including onychomycosis, onycholysis, nail dystrophy due to systemic amyloidosis and malignant nail tumours. Limitations of this review included the low amount of literature on this topic and non-standardized terminology used among research-ers. As onychoscopy is a relatively new technique, further studies and standardization of terminology are warranted to consolidate the role of dermoscopy in evaluating inflammatory nail disorders.
Keywords: allergic contact dermatitis; lichen planus; lichen striatus; onychotillomania; psoriasis; trachyonychia.
Conflict of interest statement
Figures





References
-
- Alkiewicz J. Trachyonychia. Ann Dermatol Venereol 1950; 10: 136–140.
-
- Starace M, Alessandrini A, Bruni F, Piraccini BM. Trachyonychia: a retrospective study of 122 patients in a period of 30 years. J Eur Acad Dermatol Venereol 2020; 34: 880–884. - PubMed
-
- Tosti A, Fanti PA, Morelli R, Bardazzi F. Trachyonychia associated with alopecia areata: a clinical and pathologic study. J Am Acad Dermatol 1991; 25: 266–270. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
