

Development and Implementation of a Multicomponent Protocol to Promote Sleep and Reduce Delirium in a Medical Intensive Care Unit
- PMID: 34490790
- PMCID: PMC8898983
- DOI: 10.1177/10600280211043278
Development and Implementation of a Multicomponent Protocol to Promote Sleep and Reduce Delirium in a Medical Intensive Care Unit
Abstract
Background: Evidence suggests that poor sleep increases risk of delirium. Because delirium is associated with poor outcomes, institutions have developed protocols to improve sleep in critically ill patients.
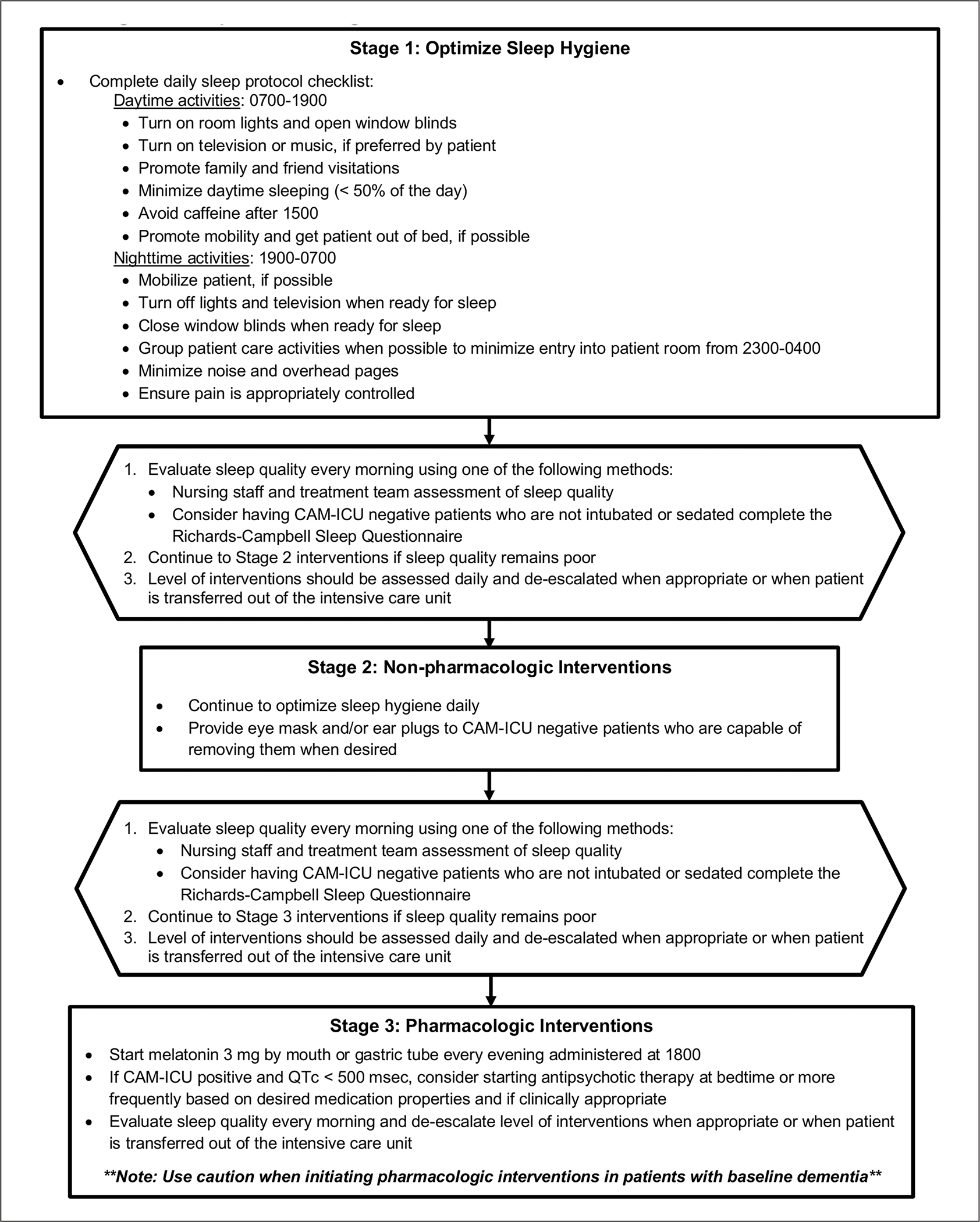
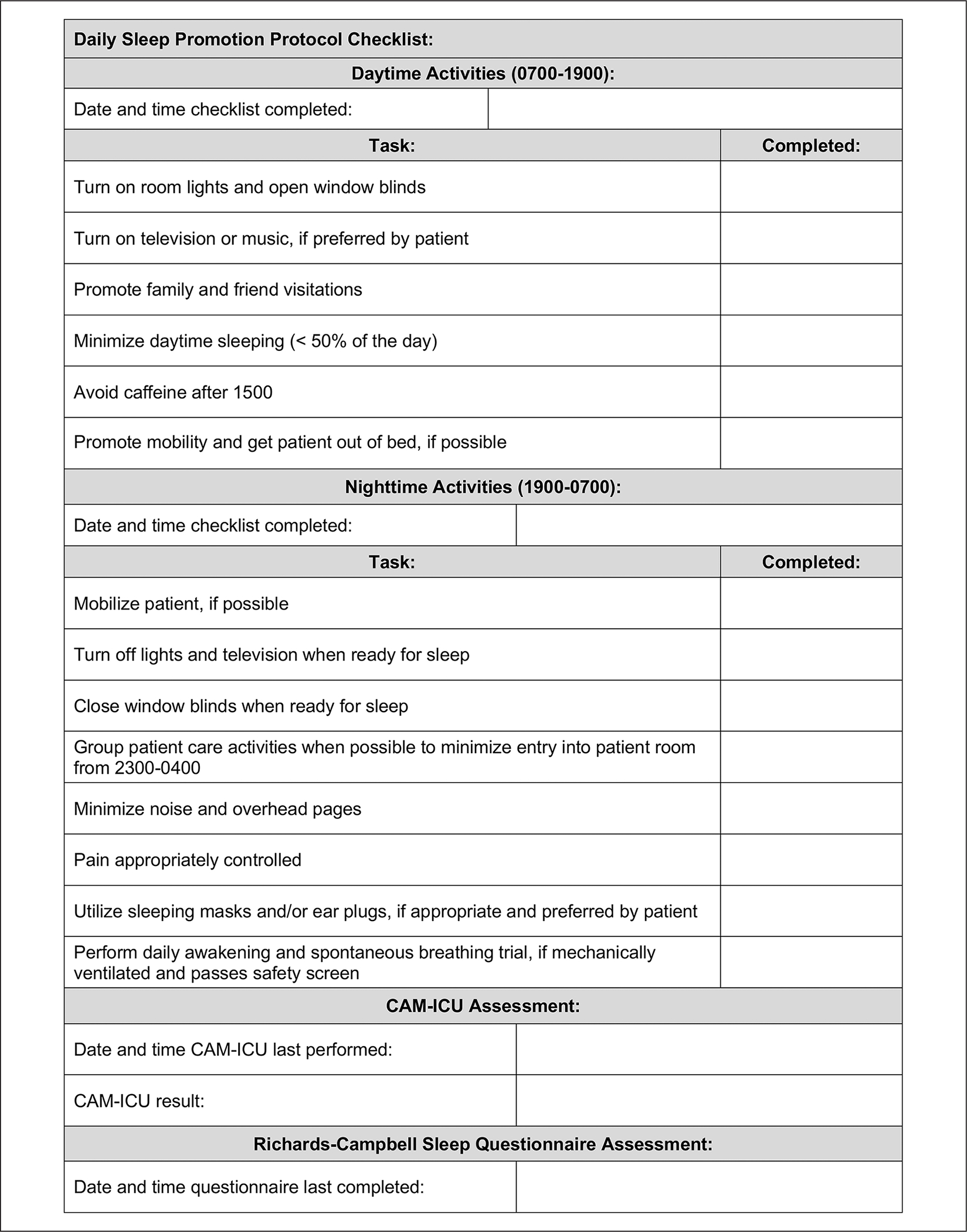
Objective: To assess the impact of implementing a multicomponent sleep protocol.
Methods: In this prospective, preimplementation and postimplementation evaluation, adult patients admitted to the medical intensive care unit (ICU) over 42 days were included. Outcomes evaluated included median delirium-free days, median Richards-Campbell Sleep Questionnaire (RCSQ) score, median optimal sleep nights, duration of mechanical ventilation (MV), ICU and hospital length of stay (LOS), and in-hospital mortality.
Results: The preimplementation group included 78 patients and postimplementation group, 84 patients. There was no difference in median delirium-free days (1 day [interquartile range, IQR, = 0-2.5] vs 1 day [IQR = 0-2]; P = 0.48), median RCSQ score (59.4 [IQR = 43.2-71.6] vs 61.2 [IQR = 49.9-75.5]; P = 0.20), median optimal sleep nights (1 night [IQR = 0-2] vs 1 night [IQR = 0-2]; P = 0.95), and in-hospital mortality (16.7% vs 17.9%, P = 1.00). Duration of MV (8 days [IQR = 4-10] vs 4 days [IQR = 2-7]; P = 0.03) and hospital LOS (13 days [IQR = 7-22.3] vs 8 days [IQR = 6-17]; P = 0.05) were shorter in the postimplementation group, but both were similar between groups after adjusting for age and severity of illness.
Conclusions and relevance: This report demonstrates that implementation of a multicomponent sleep protocol in everyday ICU care is feasible, but limitations exist when evaluating impact on measurable outcomes. Additional evaluations are needed to identify the most meaningful interventions and best practices for quantifying impact on patient outcomes.
Keywords: critical care; mechanical ventilators; quality assurance; sedatives; sleep disorders.
Conflict of interest statement
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
