

Do ScvO2 variations induced by passive leg raising predict fluid responsiveness? A prospective study
- PMID: 34491003
- PMCID: PMC8422598
- DOI: 10.14814/phy2.15012
Do ScvO2 variations induced by passive leg raising predict fluid responsiveness? A prospective study
Abstract
Objective: The present study investigates whether ScvO2 variations induced by passive leg raising (PLR) are able to predict fluid responsiveness (FR) in mechanically ventilated patients.
Design: A monocentric prospective clinical study.
Setting: An intensive care division in a tertiary hospital.
Patients: The inclusion criteria were elective postoperative cardiac surgery patients who were over 18 years old, deeply sedated, mechanically ventilated and needed volume expansion (VE). Fluid responders (R) were defined as patients who increased their left ventricular outflow tract velocity time integral (VTI) ≥15% after VE.
Intervention: In patients included in this study, continuous ScvO2 monitoring (CeVOX device, Pulsion Medical Systems) and VTI (transthoracic echocardiography) were measured simultaneously before and during a PLR test and before and after VE (with 500 ml of saline).
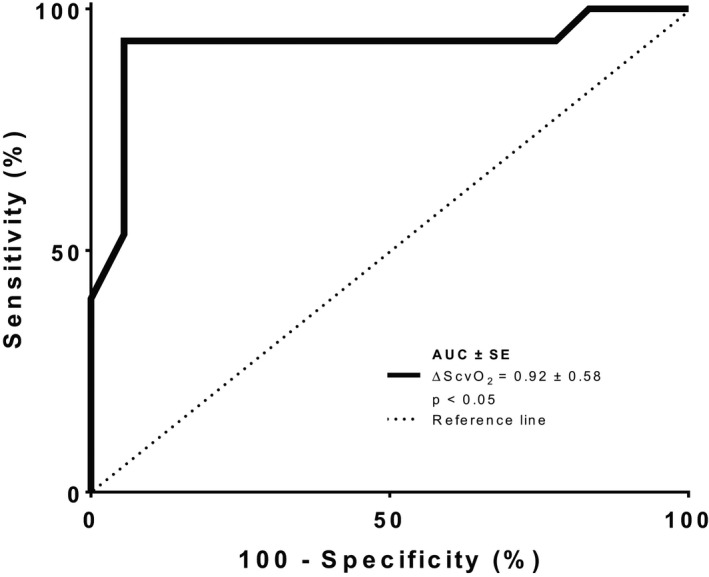
Measurements and main results: Thirty-three consecutive patients were included in this study. In 15 patients with a positive PLR test (increase in VTI ≥15%), ScvO2 increased during PLR by 9 ± 4%. In the 18 patients with a negative PLR test, ScvO2 did not significantly change during PLR. VE increased ScvO2 by 9 ± 6% and 2 ± 4% in responders and nonresponders, respectively. If ScvO2 increased by >4% during the PLR test, then a positive VTI response (≥15%) was diagnosed with a sensitivity of 93% (68-99%) and a specificity of 94% (63-99%) (Area under the receiver operating characteristic curve 0.92 ± 0.58, p < 0.05). Moreover, ScvO2 variations were able to distinguish responders to VE from nonresponders to VE with a sensitivity of 87% (68-99%) and a specificity of 89% (63-99%) (Area under the receiver operating characteristic curve 0.89 ± 0.07, p < 0.05).
Conclusions: ScvO2 variation induced by PLR is a reliable, minimally invasive parameter for predicting FR at the postoperative cardiac surgery bedside of mechanically ventilated, critically ill patients.
Keywords: ScvO2; cardiac output; central venous oxygen saturation; echocardiography; fluid responsiveness; hemodynamic; passive leg raising.
© 2021 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Figures


References
-
- Bendjelid, K., Schutz, N., Suter, P. M., & Romand, J. A. (2006). Continuous cardiac output monitoring after cardiopulmonary bypass: A comparison with bolus thermodilution measurement. Intensive Care Medicine, 32(6), 919–922. - PubMed
-
- Cannesson, M., Le Manach, Y., Hofer, C. K., Goarin, J. P., Lehot, J. J., Vallet, B. et al (2011). Assessing the diagnostic accuracy of pulse pressure variations for the prediction of fluid responsiveness: A "gray zone" approach. Anesthesiology, 115(2), 231–241. 10.1097/ALN.0b013e318225b80a. - DOI - PubMed
-
- Cecconi, M., De Backer, D., Antonelli, M., Beale, R., Bakker, J., Hofer, C. et al (2014). Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Medicine, 40(12), 1795–1815. 10.1007/s00134-014-3525-z. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
