

Machine Learning Analysis of Time-Dependent Features for Predicting Adverse Events During Hemodialysis Therapy: Model Development and Validation Study
- PMID: 34491204
- PMCID: PMC8456349
- DOI: 10.2196/27098
Machine Learning Analysis of Time-Dependent Features for Predicting Adverse Events During Hemodialysis Therapy: Model Development and Validation Study
Abstract
Background: Hemodialysis (HD) therapy is an indispensable tool used in critical care management. Patients undergoing HD are at risk for intradialytic adverse events, ranging from muscle cramps to cardiac arrest. So far, there is no effective HD device-integrated algorithm to assist medical staff in response to these adverse events a step earlier during HD.
Objective: We aimed to develop machine learning algorithms to predict intradialytic adverse events in an unbiased manner.
Methods: Three-month dialysis and physiological time-series data were collected from all patients who underwent maintenance HD therapy at a tertiary care referral center. Dialysis data were collected automatically by HD devices, and physiological data were recorded by medical staff. Intradialytic adverse events were documented by medical staff according to patient complaints. Features extracted from the time series data sets by linear and differential analyses were used for machine learning to predict adverse events during HD.
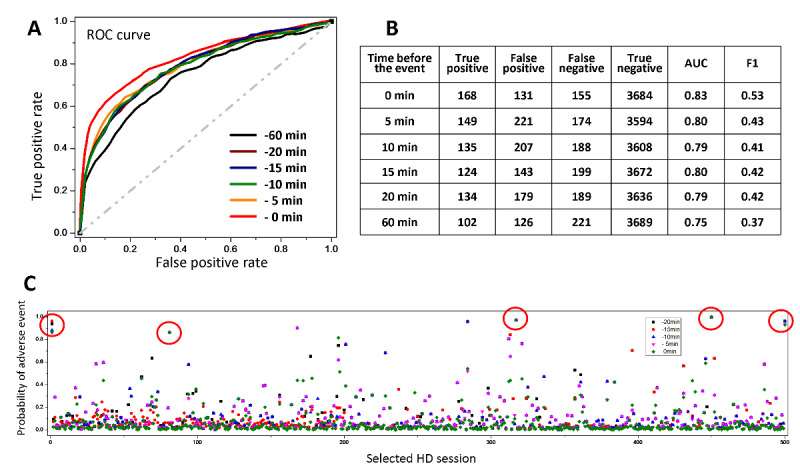
Results: Time series dialysis data were collected during the 4-hour HD session in 108 patients who underwent maintenance HD therapy. There were a total of 4221 HD sessions, 406 of which involved at least one intradialytic adverse event. Models were built by classification algorithms and evaluated by four-fold cross-validation. The developed algorithm predicted overall intradialytic adverse events, with an area under the curve (AUC) of 0.83, sensitivity of 0.53, and specificity of 0.96. The algorithm also predicted muscle cramps, with an AUC of 0.85, and blood pressure elevation, with an AUC of 0.93. In addition, the model built based on ultrafiltration-unrelated features predicted all types of adverse events, with an AUC of 0.81, indicating that ultrafiltration-unrelated factors also contribute to the onset of adverse events.
Conclusions: Our results demonstrated that algorithms combining linear and differential analyses with two-class classification machine learning can predict intradialytic adverse events in quasi-real time with high AUCs. Such a methodology implemented with local cloud computation and real-time optimization by personalized HD data could warn clinicians to take timely actions in advance.
Keywords: hemodialysis; intradialytic adverse events; machine learning; prediction algorithm.
©Yi-Shiuan Liu, Chih-Yu Yang, Ping-Fang Chiu, Hui-Chu Lin, Chung-Chuan Lo, Alan Szu-Han Lai, Chia-Chu Chang, Oscar Kuang-Sheng Lee. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 07.09.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures



Similar articles
-
Personalized prediction of intradialytic hypotension in clinical practice: Development and evaluation of a novel AI dashboard incorporating risk factors from previous and current dialysis sessions.Int J Med Inform. 2024 Oct;190:105538. doi: 10.1016/j.ijmedinf.2024.105538. Epub 2024 Jul 3. Int J Med Inform. 2024. PMID: 38968689
-
Predictive modeling of blood pressure during hemodialysis: a comparison of linear model, random forest, support vector regression, XGBoost, LASSO regression and ensemble method.Comput Methods Programs Biomed. 2020 Oct;195:105536. doi: 10.1016/j.cmpb.2020.105536. Epub 2020 May 22. Comput Methods Programs Biomed. 2020. PMID: 32485511
-
Real-time prediction of intradialytic relative blood volume: a proof-of-concept for integrated cloud computing infrastructure.BMC Nephrol. 2021 Aug 9;22(1):274. doi: 10.1186/s12882-021-02481-0. BMC Nephrol. 2021. PMID: 34372809 Free PMC article.
-
Intensive Hemodialysis and Treatment Complications and Tolerability.Am J Kidney Dis. 2016 Nov;68(5S1):S43-S50. doi: 10.1053/j.ajkd.2016.05.021. Am J Kidney Dis. 2016. PMID: 27772642 Review.
-
Prediction of intradialytic hypotension by machine learning: A systematic review.J Nephrol. 2025 May 3. doi: 10.1007/s40620-025-02288-4. Online ahead of print. J Nephrol. 2025. PMID: 40317447 Review.
Cited by
-
IRIME: Mitigating exploitation-exploration imbalance in RIME optimization for feature selection.iScience. 2024 Jul 22;27(8):110561. doi: 10.1016/j.isci.2024.110561. eCollection 2024 Aug 16. iScience. 2024. PMID: 39165845 Free PMC article.
-
Data-driven, two-stage machine learning algorithm-based prediction scheme for assessing 1-year and 3-year mortality risk in chronic hemodialysis patients.Sci Rep. 2023 Dec 5;13(1):21453. doi: 10.1038/s41598-023-48905-9. Sci Rep. 2023. PMID: 38052875 Free PMC article.
-
Early prediction of hemodialysis complications employing ensemble techniques.Biomed Eng Online. 2022 Oct 11;21(1):74. doi: 10.1186/s12938-022-01044-0. Biomed Eng Online. 2022. PMID: 36221077 Free PMC article.
-
Single-Cell RNA Sequencing Integrated with Bulk-RNA Sequencing Analysis Reveals Prognostic Signatures Based on PANoptosis in Hepatocellular Carcinoma.J Hepatocell Carcinoma. 2025 Jul 29;12:1661-1676. doi: 10.2147/JHC.S533777. eCollection 2025. J Hepatocell Carcinoma. 2025. PMID: 40761429 Free PMC article.
-
Explainable Machine Learning Techniques To Predict Amiodarone-Induced Thyroid Dysfunction Risk: Multicenter, Retrospective Study With External Validation.J Med Internet Res. 2023 Feb 7;25:e43734. doi: 10.2196/43734. J Med Internet Res. 2023. PMID: 36749620 Free PMC article.
References
-
- Ricci Z, Romagnoli S. Renal replacement therapy for critically ill patients: an intermittent continuity. Crit Care. 2014 Mar 05;18(2):115. doi: 10.1186/cc13756. https://ccforum.biomedcentral.com/articles/10.1186/cc13756 cc13756 - DOI - DOI - PMC - PubMed
-
- Douvris A, Malhi G, Hiremath S, McIntyre L, Silver SA, Bagshaw SM, Wald R, Ronco C, Sikora L, Weber C, Clark EG. Interventions to prevent hemodynamic instability during renal replacement therapy in critically ill patients: a systematic review. Crit Care. 2018 Feb 22;22(1):41. doi: 10.1186/s13054-018-1965-5. https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-1965-5 10.1186/s13054-018-1965-5 - DOI - DOI - PMC - PubMed
-
- Garzoni D, Keusch G, Kleinoeder T, Martin H, Dhondt A, Cremaschi L, Tatsis E, Ibrahim N, Boer W, Kuehne S, Claus M, Zahn M, Schuemann E, Engelmann J, Hickstein H, Wojke R, Gauly A, Passlick-Deetjen J. Reduced complications during hemodialysis by automatic blood volume controlled ultrafiltration. Int J Artif Organs. 2007 Jan;30(1):16–24. doi: 10.1177/039139880703000104. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
