

IgG Subclasses and Congenital Transmission of Chagas Disease
- PMID: 34491223
- PMCID: PMC8592205
- DOI: 10.4269/ajtmh.20-1524
IgG Subclasses and Congenital Transmission of Chagas Disease
Abstract
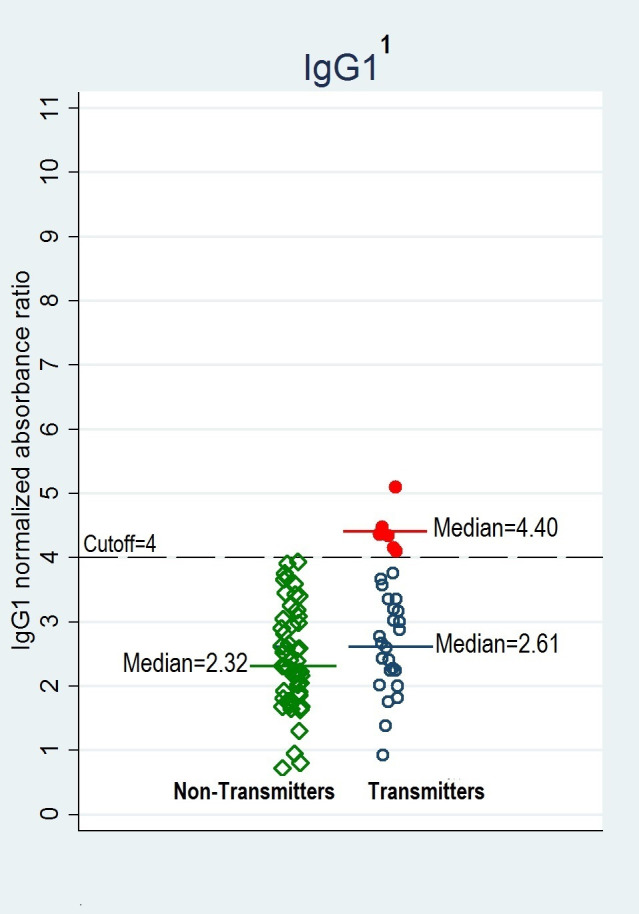
The mechanism of vertical transmission of Trypanosoma cruzi is poorly understood. In this study, we evaluated the role of IgG subclasses in the congenital transmission of Chagas disease. We conducted a case-control study in a public maternity hospital in Santa Cruz, Bolivia, enrolling women at delivery. Thirty women who transmitted T. cruzi to their newborns (cases), and 51 women who did not (controls) were randomly selected from 676 total seropositive women. Trypanosoma cruzi-specific IgG1, IgG2, and IgG3 levels were measured by in-house ELISA. The IgG4 levels were unmeasurable as a result of low levels in all participants. Quantitative polymerase chain reaction results and demographic factors were also analyzed. One-unit increases in normalized absorbance ratio of IgG1 or IgG2 levels increased the odds of congenital T. cruzi transmission in Chagas-seropositive women by 2.0 (95% CI: 1.1-3.6) and 2.27 (95% CI: 0.9-5.7), adjusted for age and previous blood transfusion. Odds of congenital transmission were 7.0 times higher in parasitemic mothers (95% CI: 2.3-21.3, P < 0.01) compared with nonparasitemic mothers. We observed that all mothers with IgG1 ≥ 4 were transmitters (sensitivity = 20%, specificity = 100%). Additionally, no mothers with IgG2 < 1.13 were transmitters (sensitivity = 100%, specificity = 21.6%). We demonstrated that IgG subclasses and parasite presence in blood are associated with vertical transmission of T. cruzi and could identify women at increased risk for congenital transmission by measuring IgG subclasses. These measures have potential as objective screening tests to predict the congenital transmission of Chagas.
Figures
References
-
- Rassi A, Rassi A, Marin-Neto JA, 2010. Chagas disease. Lancet 375: 1388–1402. - PubMed
-
- World Health Organization , 2008. Chagas Disease (American trypanosomiasis) Factsheet. Geneva, Switzerland: WHO.
-
- Coura JR, Dias JCP, 2009. Epidemiology, control and surveillance of Chagas disease: 100 years after its discovery. Mem Inst Oswaldo Cruz 104: 31–40. - PubMed
-
- Coura JR. et al. , 2002. Control of Chagas Disease. Geneva, Switzerland: World Health Organization—Technical Report Series, 1–99. - PubMed
-
- Longo DL, Bern C, 2015. Chagas’ disease. N Engl J Med 373: 456–466. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
