

Worldwide differences in primary prevention implantable cardioverter defibrillator utilization and outcomes in hypertrophic cardiomyopathy
- PMID: 34491319
- PMCID: PMC8497072
- DOI: 10.1093/eurheartj/ehab598
Worldwide differences in primary prevention implantable cardioverter defibrillator utilization and outcomes in hypertrophic cardiomyopathy
Abstract
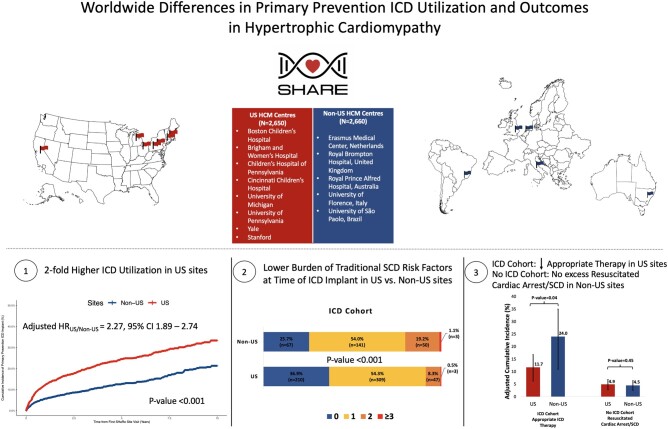
Aims: Risk stratification algorithms for sudden cardiac death (SCD) in hypertrophic cardiomyopathy (HCM) and regional differences in clinical practice have evolved over time. We sought to compare primary prevention implantable cardioverter defibrillator (ICD) implantation rates and associated clinical outcomes in US vs. non-US tertiary HCM centres within the international Sarcomeric Human Cardiomyopathy Registry.
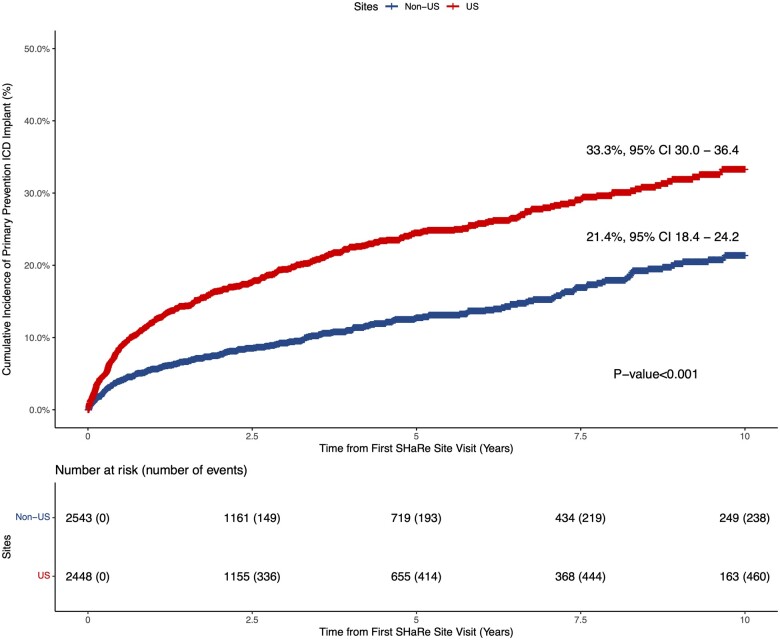
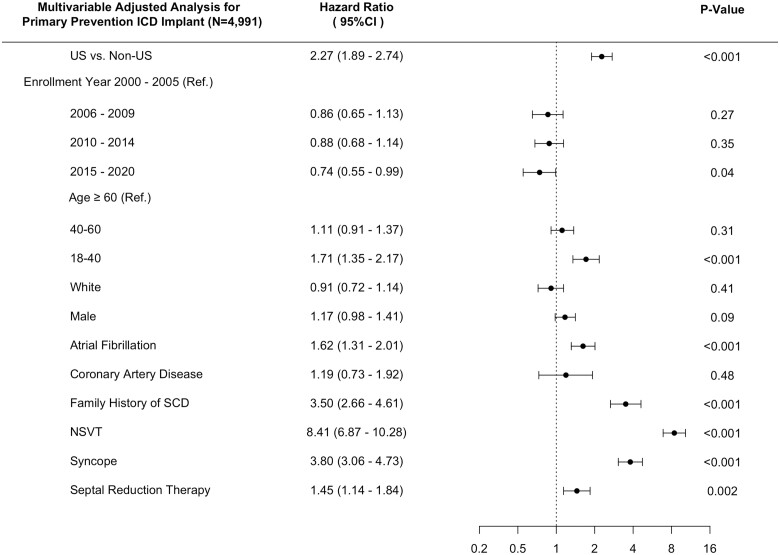
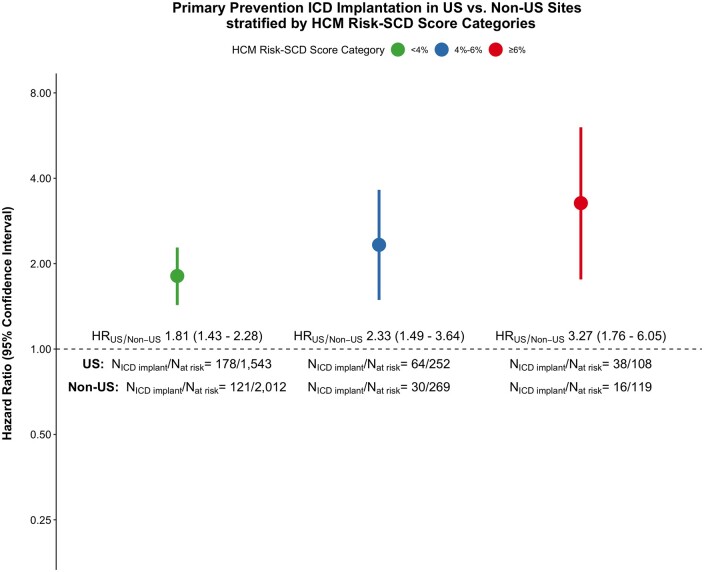
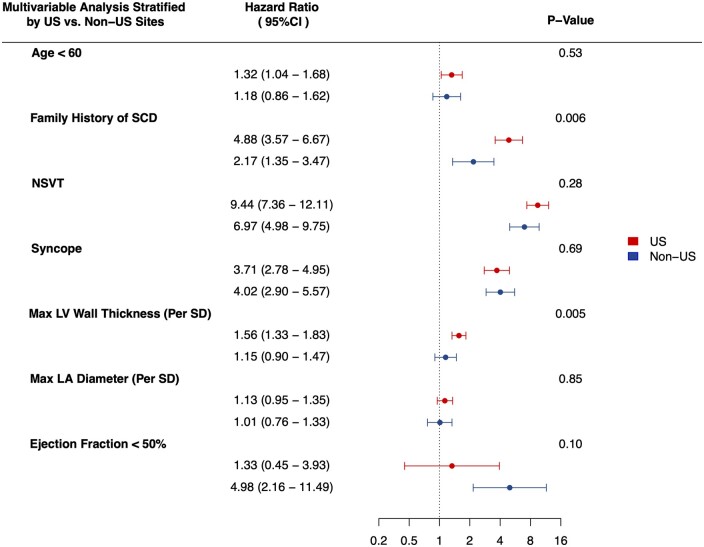
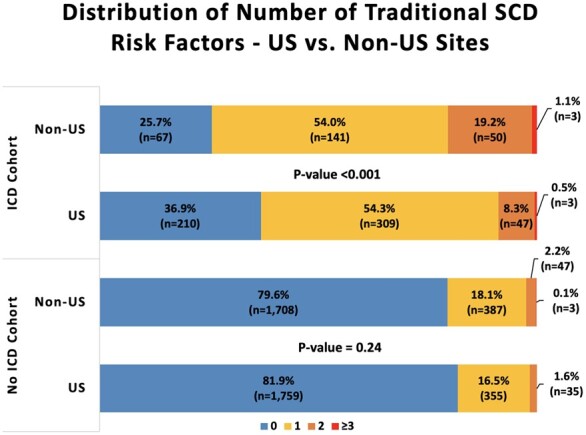
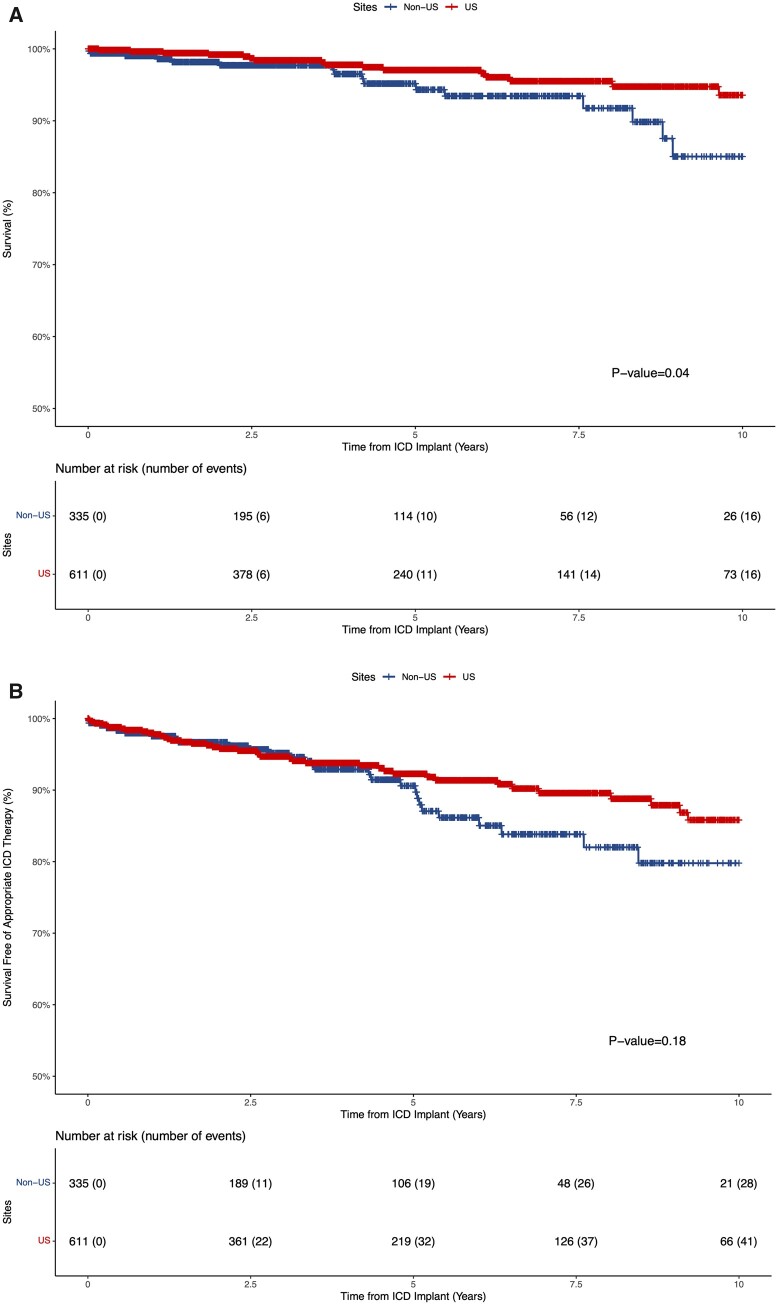
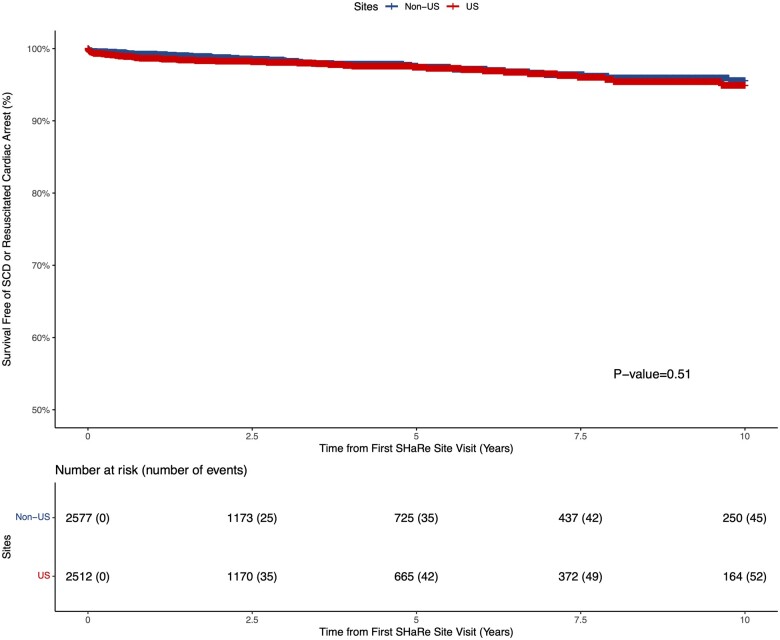
Methods and results: We included patients with HCM enrolled from eight US sites (n = 2650) and five non-US (n = 2660) sites and used multivariable Cox-proportional hazards models to compare outcomes between sites. Primary prevention ICD implantation rates in US sites were two-fold higher than non-US sites (hazard ratio (HR) 2.27 [1.89-2.74]), including in individuals deemed at high 5-year SCD risk (≥6%) based on the HCM risk-SCD score (HR 3.27 [1.76-6.05]). US ICD recipients also had fewer traditional SCD risk factors. Among ICD recipients, rates of appropriate ICD therapy were significantly lower in US vs. non-US sites (HR 0.52 [0.28-0.97]). No significant difference was identified in the incidence of SCD/resuscitated cardiac arrest among non-recipients of ICDs in US vs. non-US sites (HR 1.21 [0.74-1.97]).
Conclusion: Primary prevention ICDs are implanted more frequently in patients with HCM in US vs. non-US sites across the spectrum of SCD risk. There was a lower rate of appropriate ICD therapy in US sites, consistent with a lower-risk population, and no significant difference in SCD in US vs. non-US patients who did not receive an ICD. Further studies are needed to understand what drives malignant arrhythmias, optimize ICD allocation, and examine the impact of different ICD utilization strategies on long-term outcomes in HCM.
Keywords: Hypertrophic cardiomyopathy; Implantable cardioverter defibrillator; Outcomes; Primary prevention; Risk stratification; Sudden cardiac death.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Sudden cardiac death in hypertrophic cardiomyopathy: time to change the narrative.Eur Heart J. 2021 Oct 7;42(38):3945-3947. doi: 10.1093/eurheartj/ehab608. Eur Heart J. 2021. PMID: 34514508 No abstract available.
References
-
- Maron BJ. Clinical course and management of hypertrophic cardiomyopathy. N Engl J Med 2018;379:655–668. - PubMed
-
- Maron BJ, Shen WK, Link MS, Epstein AE, Almquist AK, Daubert JP, Bardy GH, Favale S, Rea RF, Boriani G, Estes NM 3rd, Spirito P. Efficacy of implantable cardioverter-defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med 2000;342:365–373. - PubMed
-
- O'Mahony C, Lambiase PD, Quarta G, Cardona M, Calcagnino M, Tsovolas K, Al-Shaikh S, Rahman SM, Arnous S, Jones S, McKenna W, Elliott P. The long-term survival and the risks and benefits of implantable cardioverter defibrillators in patients with hypertrophic cardiomyopathy. Heart 2012;98:116–125. - PubMed
-
- Kanterakis A, Sharma S. Cardiomyopathy and heart failure conventional risk factors for SCD in HCM. Eur Cardiol Rev 2015;10:31–36.
-
- Maron B, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH 3rd, Spirito P, Ten Cate FJ, Wigle ED; American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents; European Society of Cardiology Committee for Practice Guidelines American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. Eur Heart J 2003;24:1965–1991. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
