

The role of surgical flap design (minimally invasive flap vs. extended flap with papilla preservation) on the healing of intrabony defects treated with an enamel matrix derivative: a 12-month two-center randomized controlled clinical trial
- PMID: 34491446
- PMCID: PMC8816368
- DOI: 10.1007/s00784-021-04155-5
The role of surgical flap design (minimally invasive flap vs. extended flap with papilla preservation) on the healing of intrabony defects treated with an enamel matrix derivative: a 12-month two-center randomized controlled clinical trial
Abstract
Objectives: Minimally invasive flap designs have been introduced to enhance blood clot stability and support wound healing. Limited data appear to suggest, that in intrabony defects, better clinical outcomes can be achieved by means of minimally invasive flap compared to more extended flaps. The aim of this study was to evaluate the healing of intrabony defects treated with either minimally invasive surgical flaps or with modified or simplified papilla preservation techniques in conjunction with the application of an enamel matrix derivative (EMD).
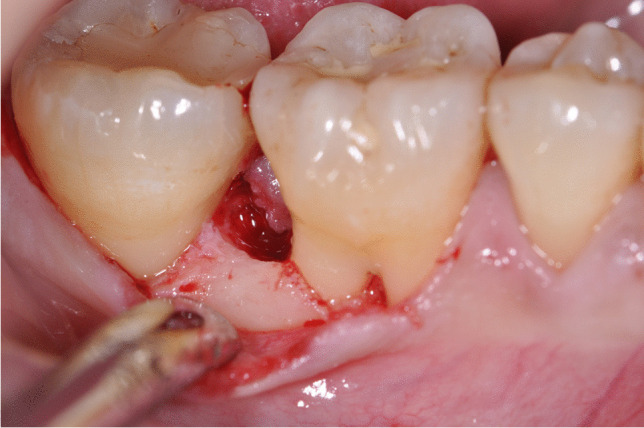
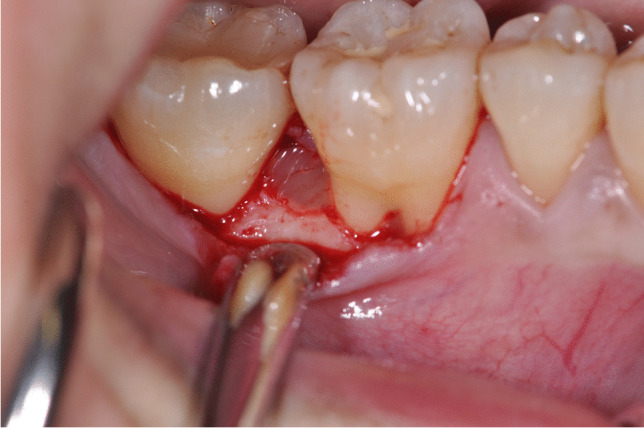
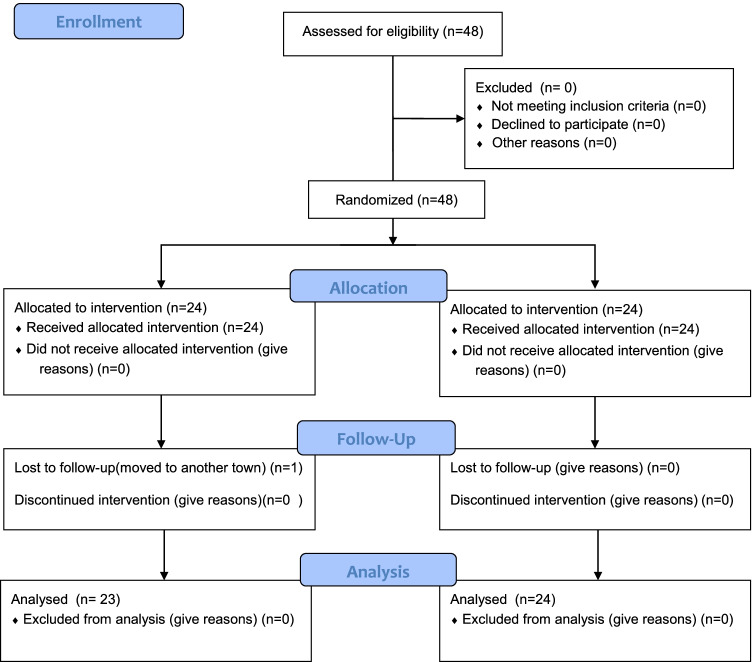
Materials and methods: Forty-seven subjects were randomly assigned to either test (N = 23) or control (N = 24) procedures. In the test group, the intrabony defects were accessed by means of either minimally invasive surgical technique (MIST) or modified minimally invasive surgical technique (M-MIST) according to the defect localization while the defects in the control group were treated with either the modified or simplified papilla preservation (MPP) or the simplified papilla preservation technique (SPP). EMD was used as regenerative material in all defects. The following clinical parameters were recorded at baseline and after 12 months: full-mouth plaque score (FMPS), full-mouth bleeding score (FMBS), probing depths (PD), clinical attachment level (CAL), and gingival recession (GR). Early healing index (EHI) score was assessed in both groups 1 week following the surgery. CAL gain was set as primary outcome.
Results: After 12 months follow-up, the CAL gain was 4.09 ± 1.68 mm in test group and 3.79 ± 1.67 mm in control group, while the PD reduction was 4.52 ± 1.34 mm and 4.04 ± 1.62 mm for test and control sites. In both groups, a minimal GR increase (0.35 ± 1.11 mm and 0.25 ± 1.03 mm) was noted. No residual PDs ≥ 6 mm were recorded in both groups. CAL gains of 4-5 mm were achieved in 30.4% and in 29.2% of test and control group, respectively. Moreover, CAL gains ≥ 6 mm were recorded in 21.7% of experimental sites and in 20.8% of control sites. No statistically significant differences in any of the evaluated parameters were found between the test and control procedures (P > 0.05). After 1 week post-surgery, a statistically significant difference (P < 0.05) between the groups was found in terms of EHI score.
Conclusions: Within the limits of this pilot RCT, the results have failed to show any differences in the measured parameters following treatment of intrabony defects with EMD, irrespective of the employed surgical technique.
Clinical relevance: In intrabony defects, the application of EMD in conjunction with either MIST/M-MIST or M-PPT/SPPT resulted in substantial clinical improvements.
Keywords: Enamel matrix derivative; Intrabony defects; Minimally invasive flaps; Periodontal disease; Randomized controlled trial; Surgical periodontal therapy; Wound healing.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Microsurgical access flap and enamel matrix derivative for the treatment of periodontal intrabony defects: a controlled clinical study.J Clin Periodontol. 2003 Jun;30(6):496-504. doi: 10.1034/j.1600-051x.2003.00013.x. J Clin Periodontol. 2003. PMID: 12795787 Clinical Trial.
-
Enamel matrix proteins in the regenerative therapy of deep intrabony defects.J Clin Periodontol. 2002 Apr;29(4):317-25. doi: 10.1034/j.1600-051x.2002.290407.x. J Clin Periodontol. 2002. PMID: 11966929 Clinical Trial.
-
Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: a 24-month randomized controlled clinical trial.Clin Oral Investig. 2021 Aug;25(8):5095-5107. doi: 10.1007/s00784-021-03822-x. Epub 2021 Feb 10. Clin Oral Investig. 2021. PMID: 33565017 Free PMC article. Clinical Trial.
-
Effect of Flap Design for Enamel Matrix Derivative Application in Intraosseous Defects.JDR Clin Trans Res. 2021 Apr;6(2):184-194. doi: 10.1177/2380084420934731. Epub 2020 Jun 19. JDR Clin Trans Res. 2021. PMID: 32559395
-
Minimally invasive periodontal regeneration with the buccal approach: a systematic review and meta-analysis of clinical studies.Evid Based Dent. 2024 Mar;25(1):54. doi: 10.1038/s41432-023-00964-7. Epub 2024 Jan 5. Evid Based Dent. 2024. PMID: 38182662
Cited by
-
Single-flap approach versus without concentrate growth factor in the treatment of periodontal supra-osseous defects: A randomized controlled clinical trial.Saudi Dent J. 2024 Feb;36(2):328-333. doi: 10.1016/j.sdentj.2023.11.015. Epub 2023 Nov 15. Saudi Dent J. 2024. PMID: 38419996 Free PMC article.
-
Beyond traditional diagnosis: aptamer-based microRNA detection for the early diagnosis of periodontitis.Mol Biol Rep. 2025 Jun 16;52(1):604. doi: 10.1007/s11033-025-10676-z. Mol Biol Rep. 2025. PMID: 40523972 Review.
-
Do patient and surgical factors predict postoperative discomfort in implant dentistry?Evid Based Dent. 2025 Mar;26(1):23-25. doi: 10.1038/s41432-025-01122-x. Epub 2025 Feb 11. Evid Based Dent. 2025. PMID: 39934387
-
Fabrication and Characterization of a Stretchable Sodium Alginate Hydrogel Patch Combined with Silicon Nitride and Metalized Halloysite Nanotubes to Develop a Chronic Wound Healing Treatment.Int J Mol Sci. 2025 Feb 18;26(4):1734. doi: 10.3390/ijms26041734. Int J Mol Sci. 2025. PMID: 40004197 Free PMC article.
-
Non-Surgical Treatment of Moderate Periodontal Intrabony Defects With Adjunctive Cross-Linked Hyaluronic Acid: A Single-Blinded Randomized Controlled Clinical Trial.J Clin Periodontol. 2025 Feb;52(2):310-322. doi: 10.1111/jcpe.14078. Epub 2024 Oct 14. J Clin Periodontol. 2025. PMID: 39402910 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
