

Imaging of acute pelvic pain
- PMID: 34491817
- PMCID: PMC8553212
- DOI: 10.1259/bjr.20210281
Imaging of acute pelvic pain
Abstract
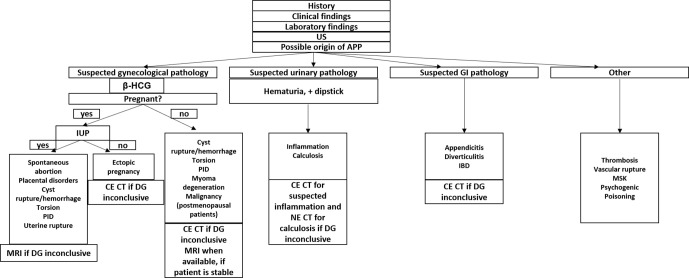
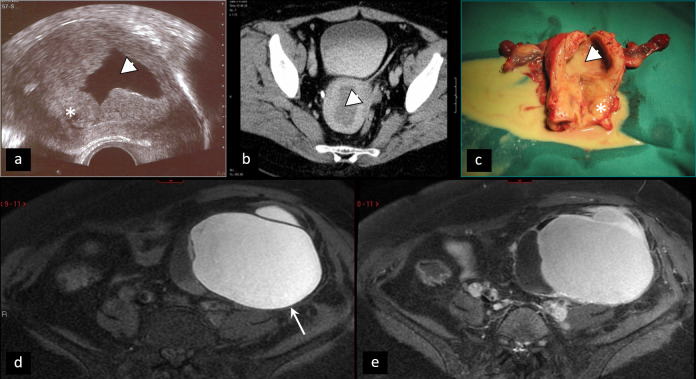
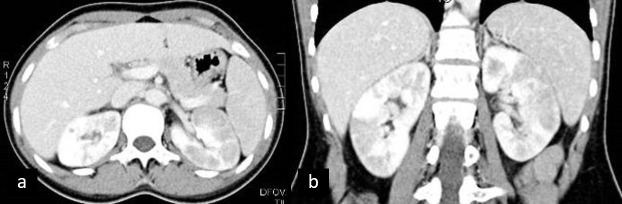
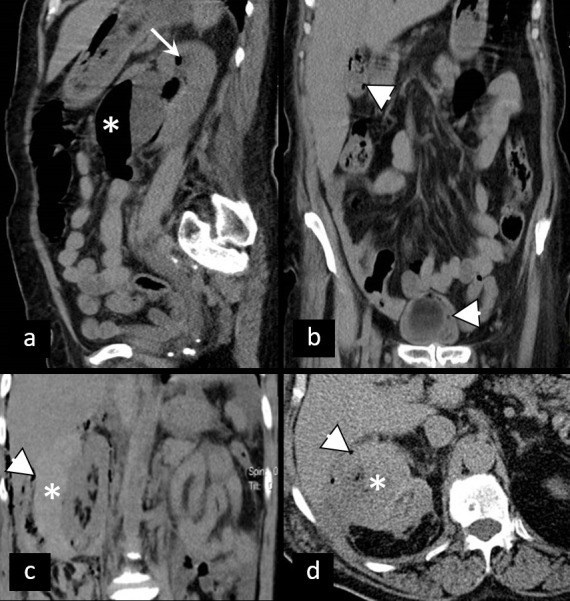
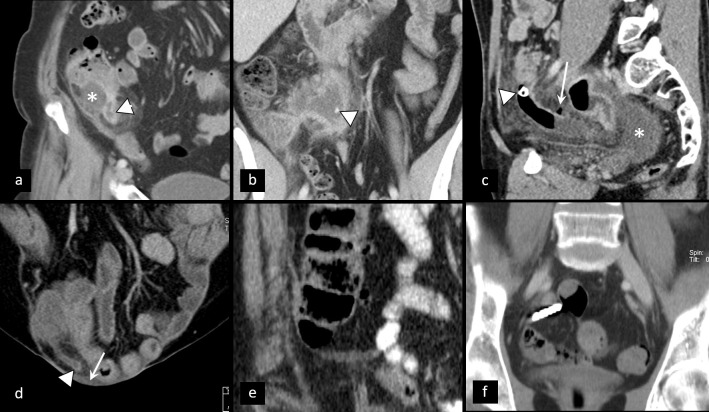
Acute pelvic pain (APP) requires urgent medical evaluation and treatment. Differential diagnosis of APP is broad, including a variety of gynecologic and non-gynecologic/ urinary, gastrointestinal, vascular and other entities. Close anatomical and physiological relations of pelvic structures, together with similar clinical presentation of different disorders and overlapping of symptoms, especially in the emergency background, make the proper diagnosis of APP challenging. Imaging plays a crucial role in the fast and precise diagnosis of APP. Ultrasonography is the first-line imaging modality, often accompanied by CT, while MRI is utilized in specific cases, using short, tailored protocols. Recognizing the cause of APP in females is a challenging task, due to the wide spectrum of possible origin and overlap of their imaging features. Therefore, the radiologist has to be familiar with the possible causes of APP, and, relying on clinical presentation, together with laboratory findings, choose the best imaging strategy in order to establish a fast and accurate diagnosis.
Figures



References
-
- Zafar N, Kupesic Plavsic S. Role of ultrasound in the evaluation of acute pelvic pain in nonpregnant reproductive age patients. Reprod Age Patients Donald Sch J Ultrasound Obs Gynecol 2012; 6: 207–17. doi: 10.5005/jp-journals-10009-1244 - DOI
-
- Alt C, Bharwani N, Brunesch L, Stanza FM, Ma D, El SRF. ESUR quick guide to female pelvis imaging. Lisboa, Portugal: ESUR; 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
