

From first to second wave: follow-up of the prospective COVID-19 cohort (KoCo19) in Munich (Germany)
- PMID: 34493217
- PMCID: PMC8423599
- DOI: 10.1186/s12879-021-06589-4
From first to second wave: follow-up of the prospective COVID-19 cohort (KoCo19) in Munich (Germany)
Abstract
Background: In the 2nd year of the COVID-19 pandemic, knowledge about the dynamics of the infection in the general population is still limited. Such information is essential for health planners, as many of those infected show no or only mild symptoms and thus, escape the surveillance system. We therefore aimed to describe the course of the pandemic in the Munich general population living in private households from April 2020 to January 2021.
Methods: The KoCo19 baseline study took place from April to June 2020 including 5313 participants (age 14 years and above). From November 2020 to January 2021, we could again measure SARS-CoV-2 antibody status in 4433 of the baseline participants (response 83%). Participants were offered a self-sampling kit to take a capillary blood sample (dry blood spot; DBS). Blood was analysed using the Elecsys® Anti-SARS-CoV-2 assay (Roche). Questionnaire information on socio-demographics and potential risk factors assessed at baseline was available for all participants. In addition, follow-up information on health-risk taking behaviour and number of personal contacts outside the household (N = 2768) as well as leisure time activities (N = 1263) were collected in summer 2020.
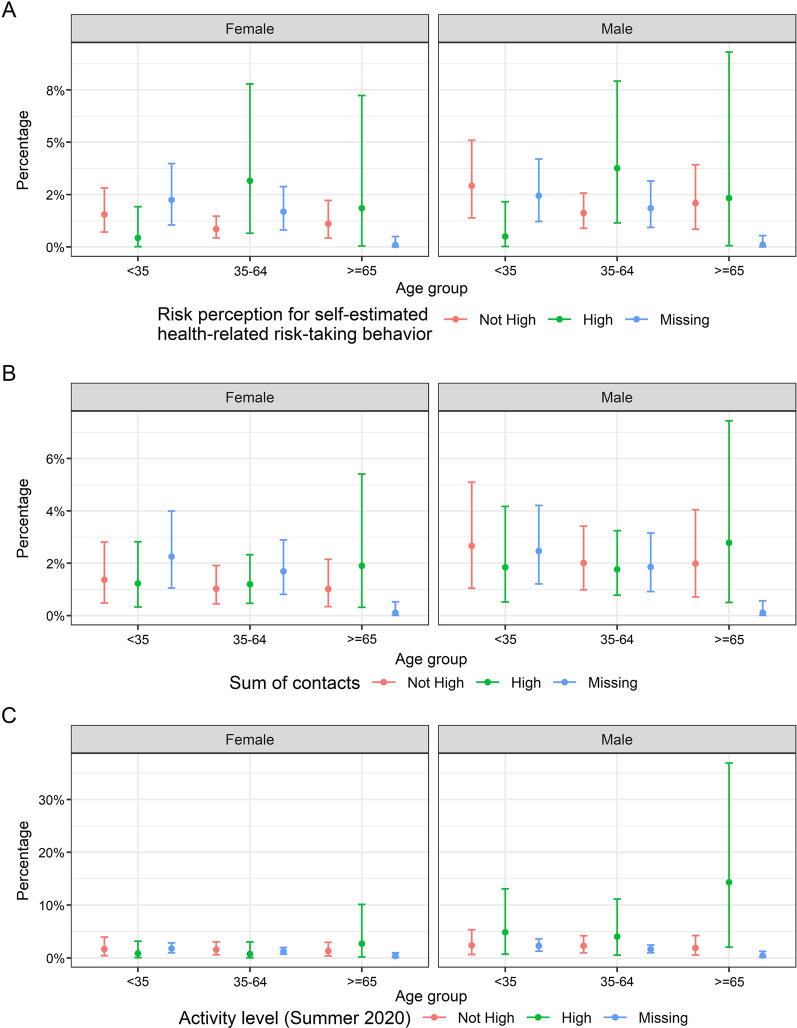
Results: Weighted and adjusted (for specificity and sensitivity) SARS-CoV-2 sero-prevalence at follow-up was 3.6% (95% CI 2.9-4.3%) as compared to 1.8% (95% CI 1.3-3.4%) at baseline. 91% of those tested positive at baseline were also antibody-positive at follow-up. While sero-prevalence increased from early November 2020 to January 2021, no indication of geospatial clustering across the city of Munich was found, although cases clustered within households. Taking baseline result and time to follow-up into account, men and participants in the age group 20-34 years were at the highest risk of sero-positivity. In the sensitivity analyses, differences in health-risk taking behaviour, number of personal contacts and leisure time activities partly explained these differences.
Conclusion: The number of citizens in Munich with SARS-CoV-2 antibodies was still below 5% during the 2nd wave of the pandemic. Antibodies remained present in the majority of SARS-CoV-2 sero-positive baseline participants. Besides age and sex, potentially confounded by differences in behaviour, no major risk factors could be identified. Non-pharmaceutical public health measures are thus still important.
Keywords: COVID-19; ORCHESTRA; Population-based cohort study; SARS-CoV-2; Sero-incidence; Sero-prevalence.
© 2021. The Author(s).
Conflict of interest statement
In addition to the funding disclosed in the funding section, DM and VT are sub-investigators vaccines trials sponsored by Curevac AG. LO received non-financial support from Dr. Box Betrobox and grants from the Bavarian State Ministry of Science and the Arts during the conduct of the study. CR received royalities from Elsevier LTD for the textbook “Clinical Cases in Tropical Medicine”. She also received honoraria for lectures done at non-private academic institutions. CR is also chair of the “Travel medicine” board of the of the German Society for the Tropical Medicine, Travel Medicine and global health (unpaid) and member of the permanent committee on vaccinations at the Robert-Koch-Institute work group on travel vaccinations (unpaid). AW is on Roche Diagnostics and Roche Pharma Advisory Boards related SARS-CoV-2. The Bundeswehr Institute of Microbiology (RW) received research funding from the Medical Biodefence program of the Bundeswehr. The funders had no role in study design, data collection, data analyses, data interpretation, writing, or submission of this manuscript.
Figures






References
-
- Olbrich L, Castelletti N, Schälte Y, Garí M, Pütz P, Bakuli A, et al. A serology strategy for epidemiological studies based on the comparison of the performance of seven different test systems—the representative COVID-19 cohort Munich. medRxiv. 2021;26:1033.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
