

The epidemiology of bloodstream infections and antimicrobial susceptibility patterns in Thuringia, Germany: a five-year prospective, state-wide surveillance study (AlertsNet)
- PMID: 34493334
- PMCID: PMC8424790
- DOI: 10.1186/s13756-021-00997-6
The epidemiology of bloodstream infections and antimicrobial susceptibility patterns in Thuringia, Germany: a five-year prospective, state-wide surveillance study (AlertsNet)
Abstract
Background: Monitoring pathogens of bloodstream infections (BSI) and their antibiotic susceptibility is important to guide empiric antibiotic treatment strategies and prevention programs. This study assessed the epidemiology of BSI and antibiotic resistance patterns at the German Federal State of Thuringia longitudinally.
Methods: A surveillance network consisting of 26 hospitals was established to monitor BSIs from 01/2015 to 12/2019. All blood culture results, without restriction of age of patients, of the participating hospitals were reported by the respective microbiological laboratory. A single detection of obligate pathogens and a repeated detection of coagulase-negative staphylococci, Bacillus spp., Corynebacterium spp., Micrococcus spp. and Propionibacterium spp., within 96 h were regarded as a relevant positive blood culture. If one of the aforementioned non-obligate pathogens has been detected only once within 96 h, contamination has been assumed. Logistic regression models were applied to analyse the relationship between resistance, year of BSI and hospital size. Generalized estimating equations were used to address potential clustering.
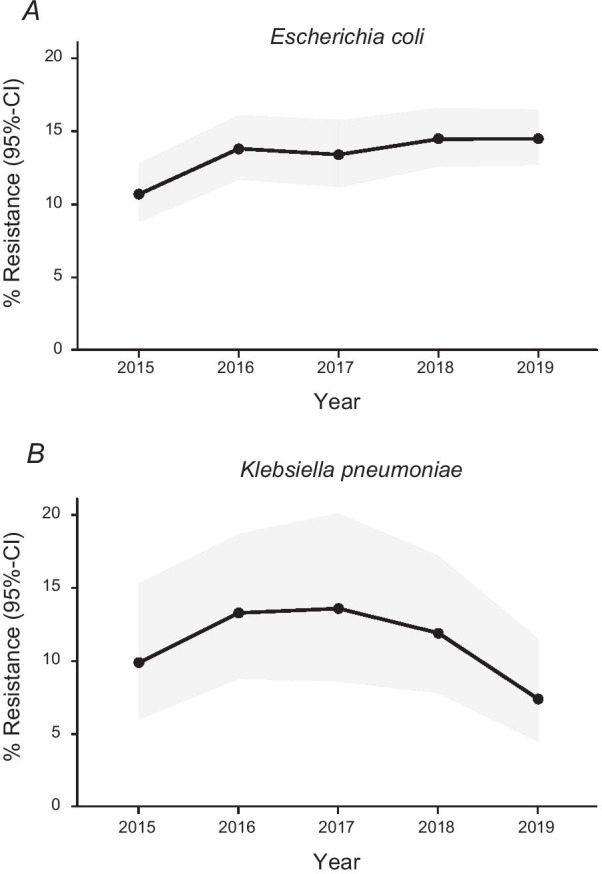
Results: A total of 343,284 blood cultures (BC) of 82,527 patients were recorded. Overall, 2.8% (n = 9571) of all BCs were classified as contaminated. At least one relevant pathogen was identified in 13.2% (n = 45,346) of BCs. Escherichia coli (25.4%) was the most commonly detected pathogen, followed by Staphylococcus aureus (15.2%), Staphylococcus epidermidis (8.1%) and Klebsiella pneumoniae (4.6%). In S. aureus, we observed a decline of methicillin resistance (MRSA) from 10.4% in 2015 to 2.5% in 2019 (p < 0.001). The rate of vancomycin resistance in Enterococcus faecium (VRE) has increased from 16.7% in 2015 to 26.9% in 2019 (p < 0.001), with a peak in 2018 (42.5%). In addition, we observed an increase of Cefotaxime (3GC) resistance in E. coli from 10.7% in 2015 to 14.5% in 2019 (p = 0.007) whereas 3GC resistance in K. pneumoniae was stable (2015: 9.9%; 2019: 7.4%, p = 0.35). Carbapenem resistance was less than 1% for both pathogens. These patterns were robustly observed across sensitivity analyses.
Conclusions: We observed evidence for a decline in MRSA, an increase in VRE and a very low rate of carbapenem resistance in gram-negative bacteria. 3GC resistance in E. coli increased constantly over time.
Keywords: Bloodstream infections; ESBL; Epidemiology; MRSA; Surveillance.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no potential financial or ethical conflicts of interest regarding the contents of the publication.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
