

Pulse oximetry adoption and oxygen orders at paediatric admission over 7 years in Kenya: a multihospital retrospective cohort study
- PMID: 34493522
- PMCID: PMC8424839
- DOI: 10.1136/bmjopen-2021-050995
Pulse oximetry adoption and oxygen orders at paediatric admission over 7 years in Kenya: a multihospital retrospective cohort study
Abstract
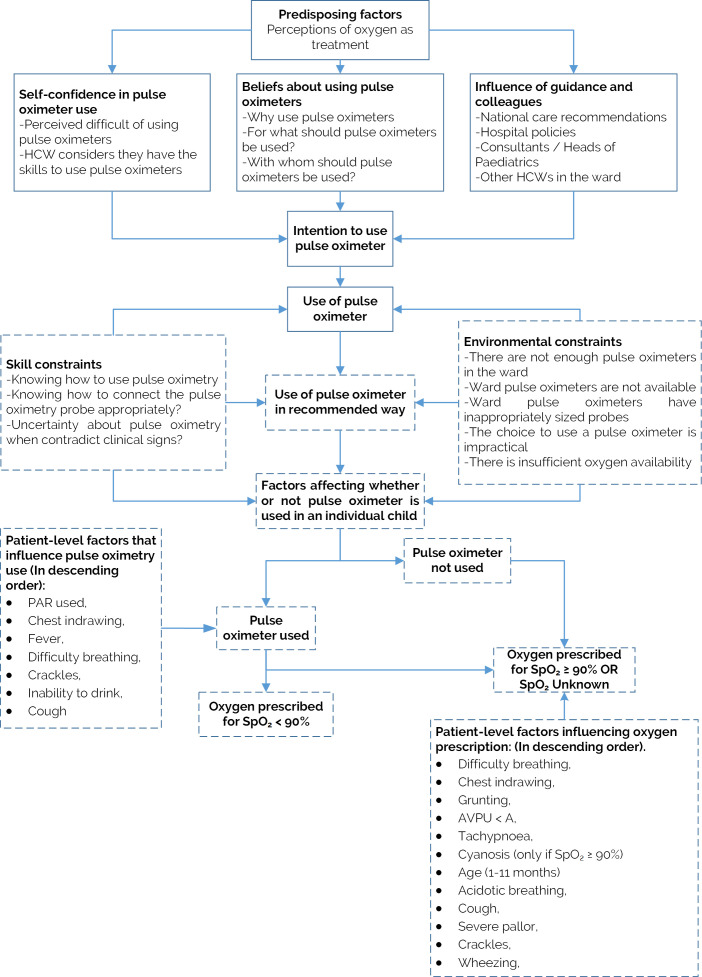
Objectives: To characterise adoption and explore specific clinical and patient factors that might influence pulse oximetry and oxygen use in low-income and middle-income countries (LMICs) over time; to highlight useful considerations for entities working on programmes to improve access to pulse oximetry and oxygen.
Design: A multihospital retrospective cohort study.
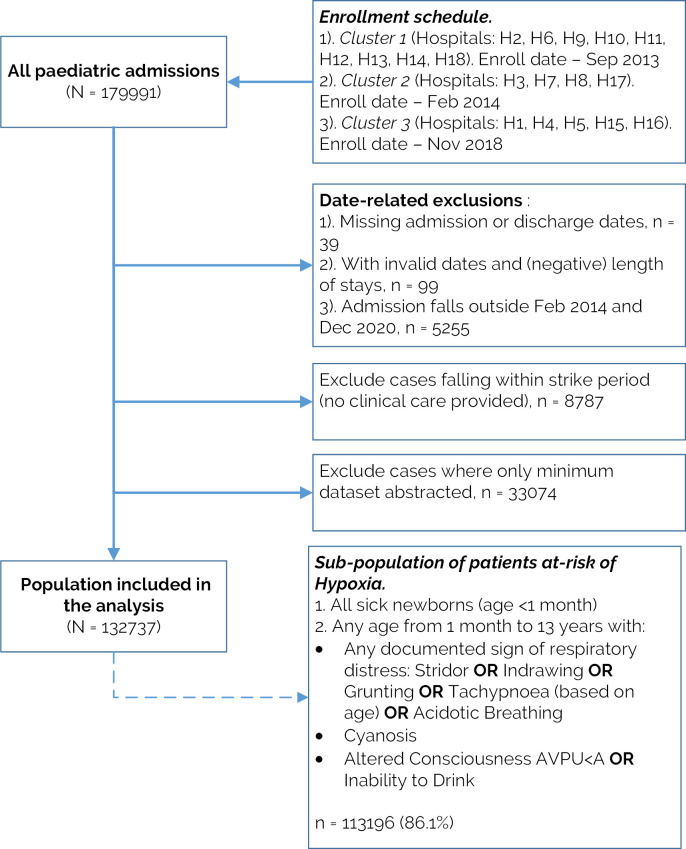
Settings: All admissions (n=132 737) to paediatric wards of 18 purposely selected public hospitals in Kenya that joined a Clinical Information Network (CIN) between March 2014 and December 2020.
Outcomes: Pulse oximetry use and oxygen prescription on admission; we performed growth-curve modelling to investigate the association of patient factors with study outcomes over time while adjusting for hospital factors.
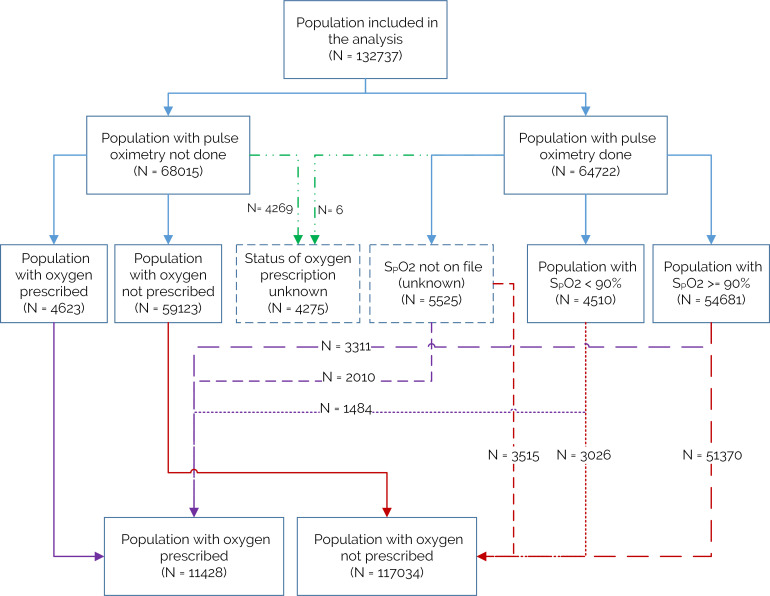
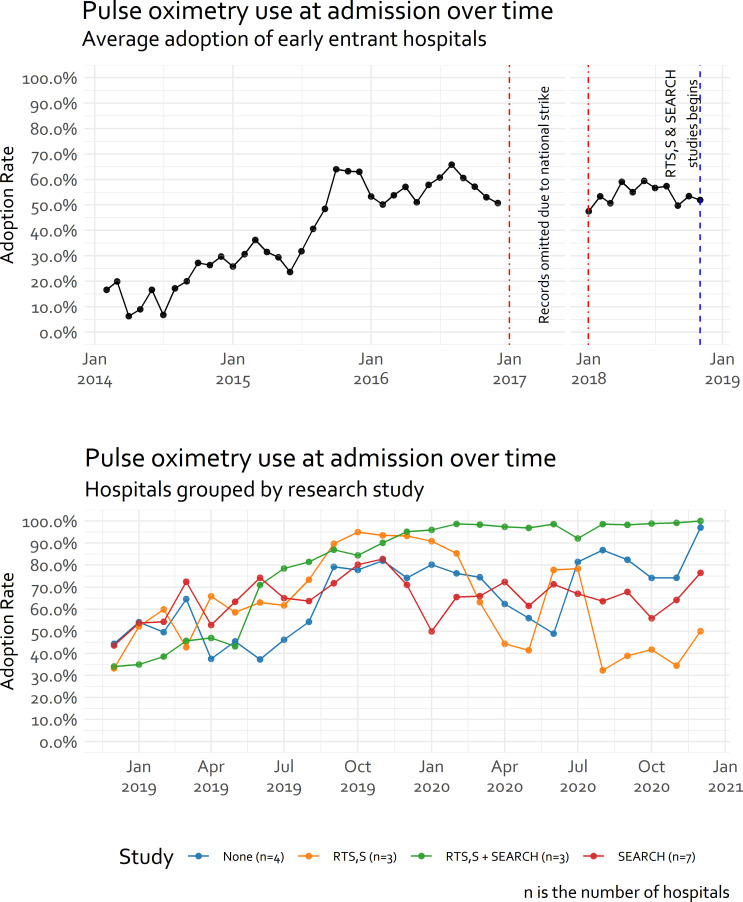
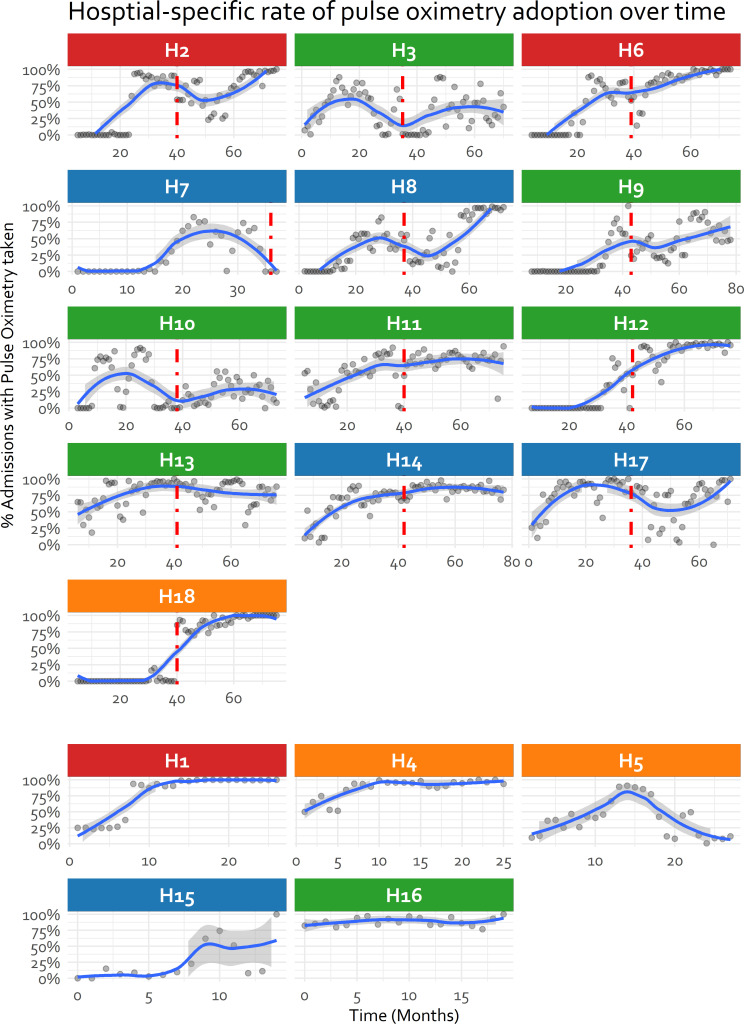
Results: Overall, pulse oximetry was used in 48.8% (64 722/132 737) of all admission cases. Use rose on average with each month of participation in the CIN (OR: 1.11, 95% CI 1.05 to 1.18) but patterns of adoption were highly variable across hospitals suggesting important factors at hospital level influence use of pulse oximetry. Of those with pulse oximetry measurement, 7% (4510/64 722) had hypoxaemia (SpO2 <90%). Across the same period, 8.6% (11 428/132 737) had oxygen prescribed but in 87%, pulse oximetry was either not done or the hypoxaemia threshold (SpO2 <90%) was not met. Lower chest-wall indrawing and other respiratory symptoms were associated with pulse oximetry use at admission and were also associated with oxygen prescription in the absence of pulse oximetry or hypoxaemia.
Conclusion: The adoption of pulse oximetry recommended in international guidelines for assessing children with severe illness has been slow and erratic, reflecting system and organisational weaknesses. Most oxygen orders at admission seem driven by clinical and situational factors other than the presence of hypoxaemia. Programmes aiming to implement pulse oximetry and oxygen systems will likely need a long-term vision to promote adoption, guideline development and adherence and continuously examine impact.
Keywords: audit; epidemiology; paediatrics; protocols & guidelines; quality in health care; tropical medicine.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization . Manual on use of oxygen therapy in children. World Health Organization, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous