

The endogenous circadian system worsens asthma at night independent of sleep and other daily behavioral or environmental cycles
- PMID: 34493686
- PMCID: PMC8449316
- DOI: 10.1073/pnas.2018486118
The endogenous circadian system worsens asthma at night independent of sleep and other daily behavioral or environmental cycles
Abstract
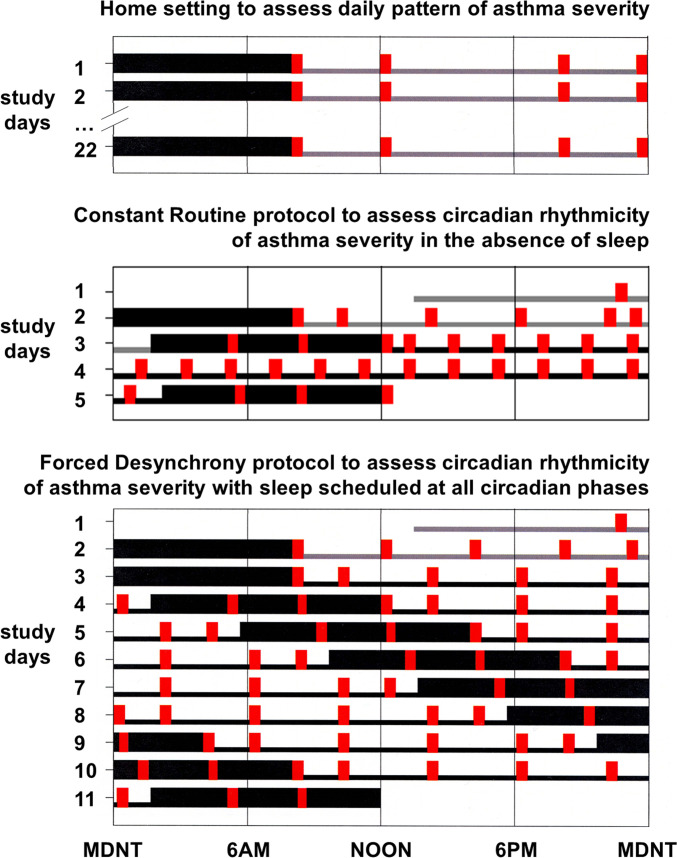
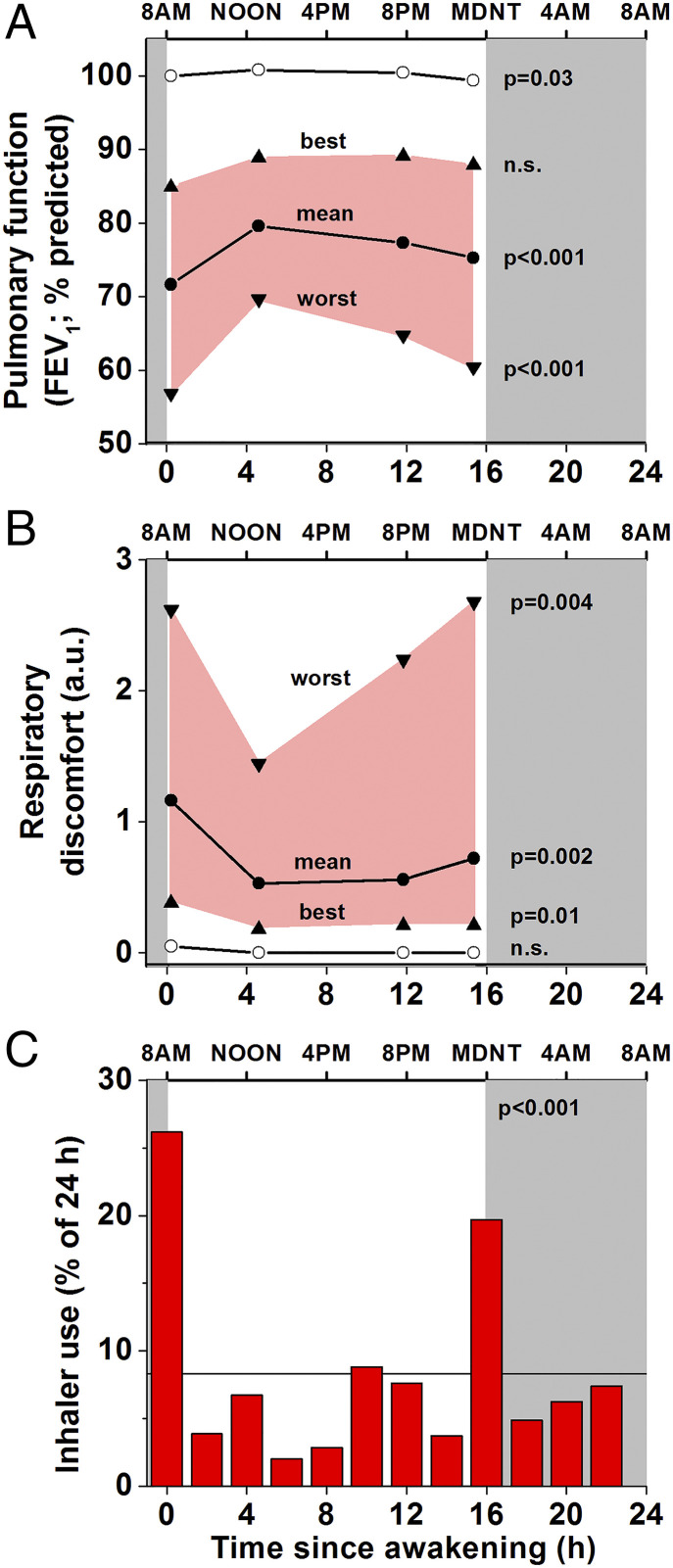
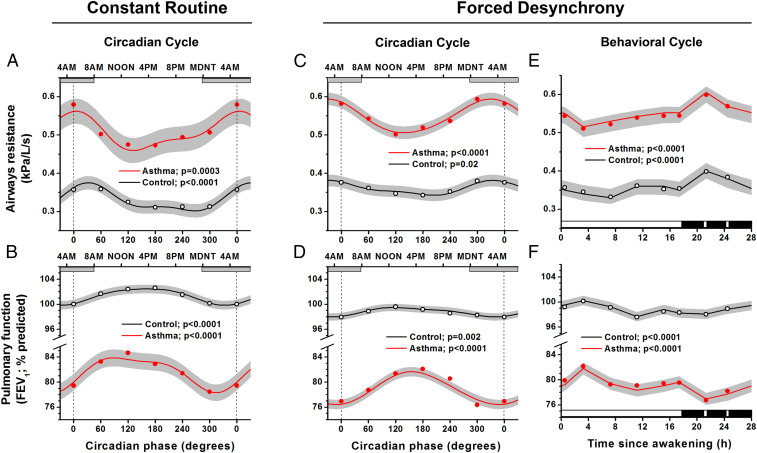
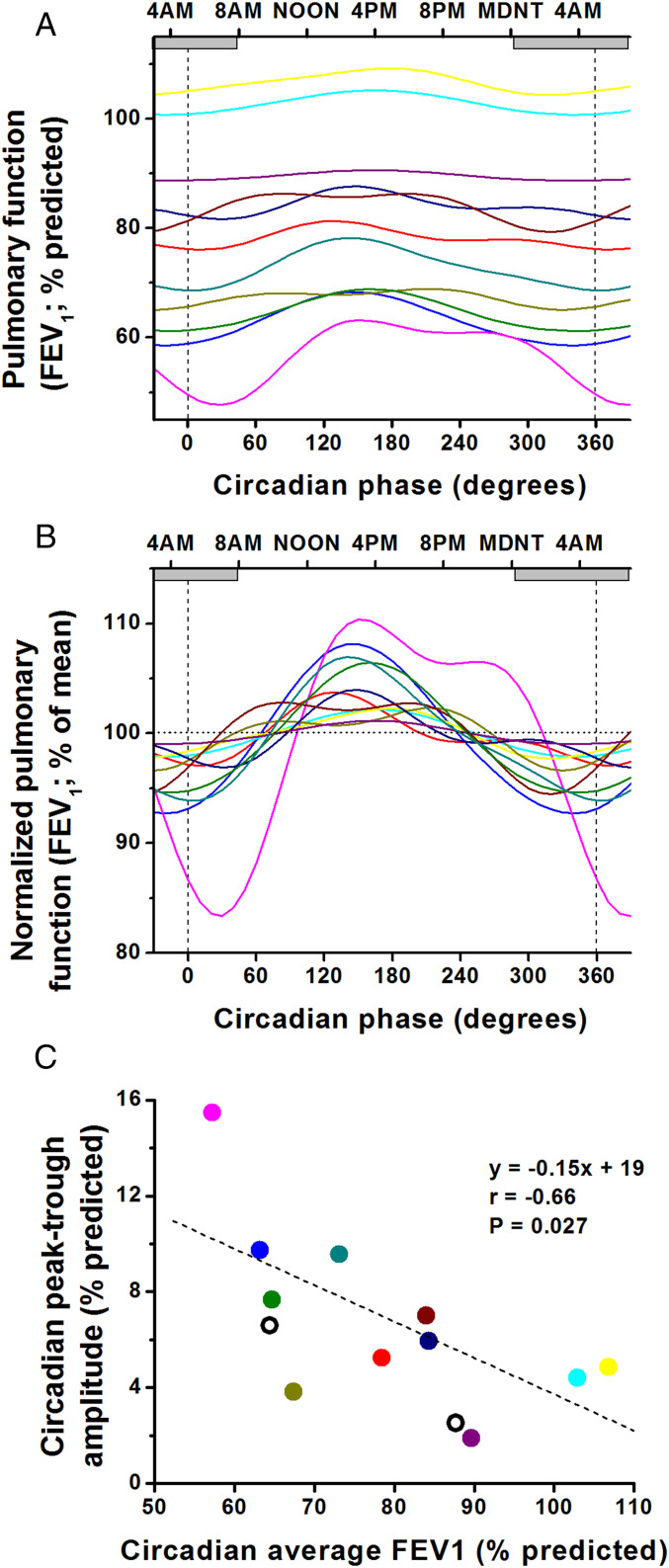
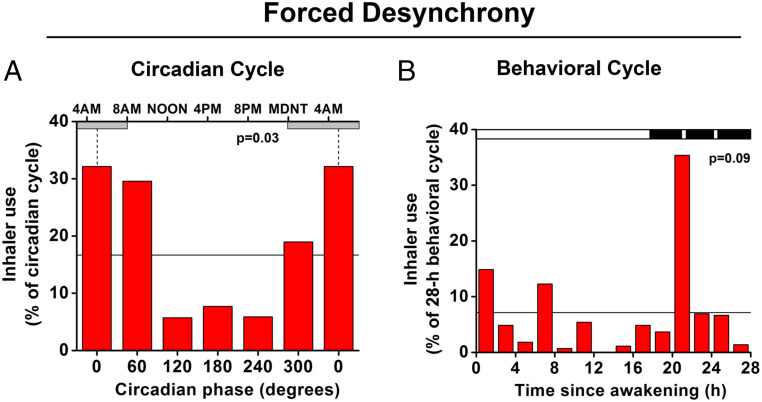
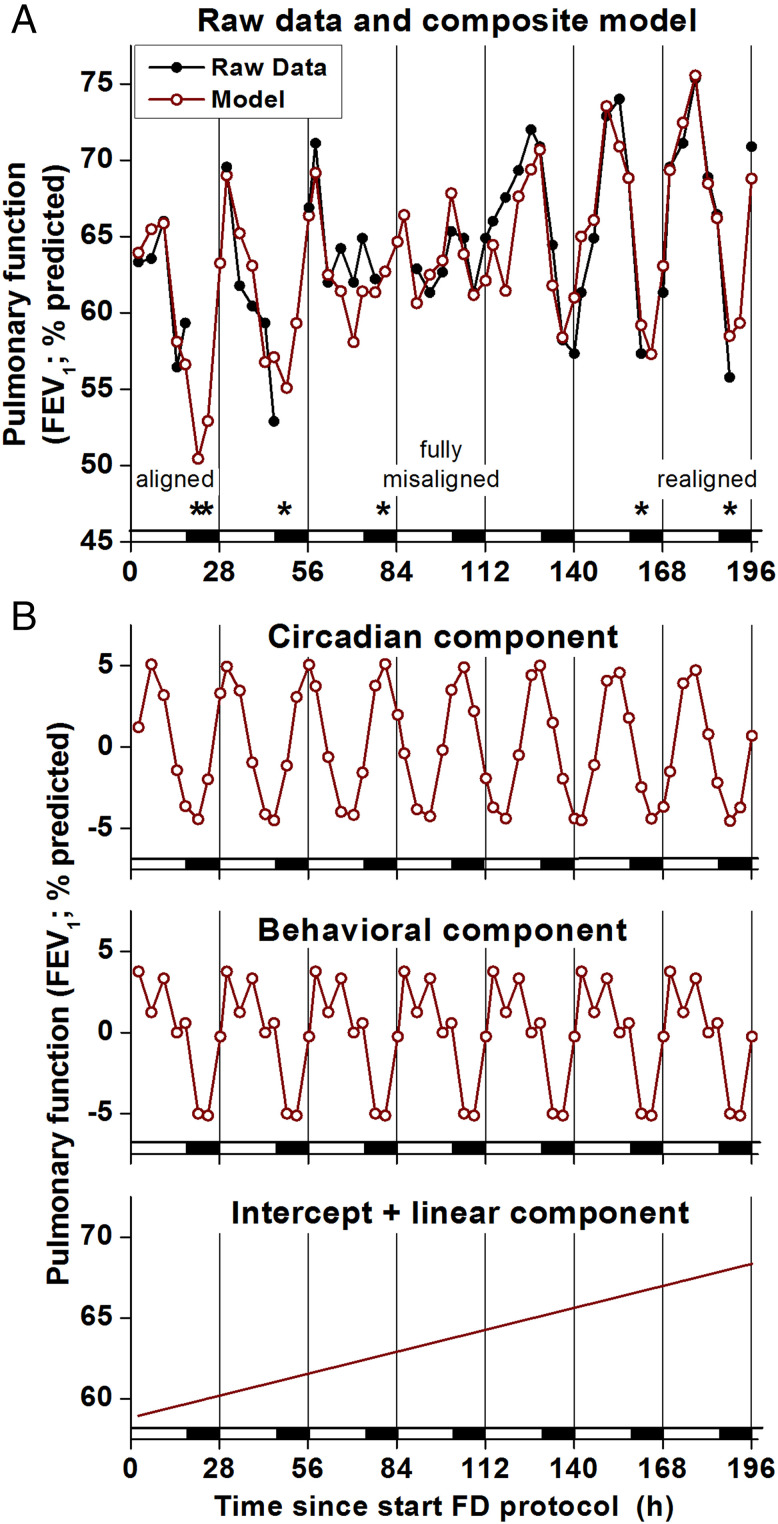
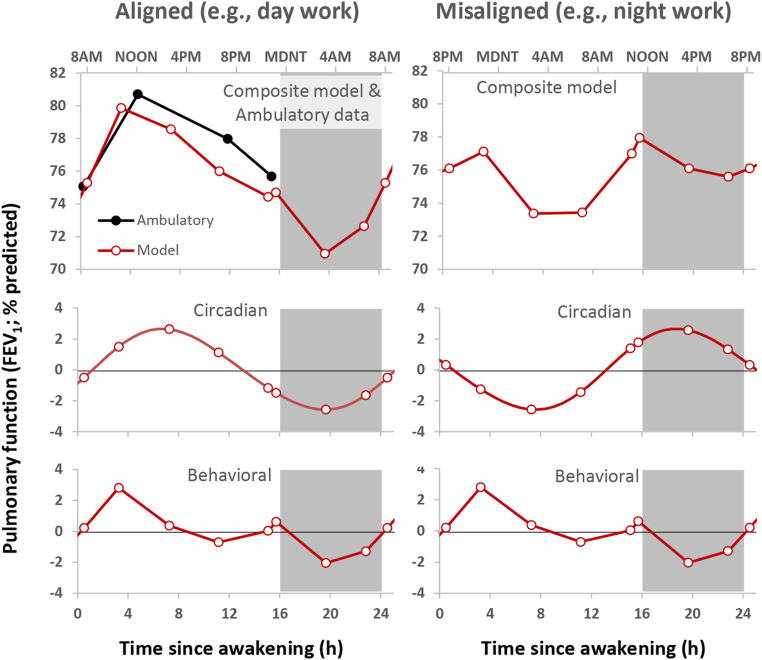
Asthma often worsens at night. To determine if the endogenous circadian system contributes to the nocturnal worsening of asthma, independent of sleep and other behavioral and environmental day/night cycles, we studied patients with asthma (without steroid use) over 3 wk in an ambulatory setting (with combined circadian, environmental, and behavioral effects) and across the circadian cycle in two complementary laboratory protocols performed in dim light, which separated circadian from environmental and behavioral effects: 1) a 38-h "constant routine," with continuous wakefulness, constant posture, 2-hourly isocaloric snacks, and 2) a 196-h "forced desynchrony" incorporating seven identical recurring 28-h sleep/wake cycles with all behaviors evenly scheduled across the circadian cycle. Indices of pulmonary function varied across the day in the ambulatory setting, and both laboratory protocols revealed significant circadian rhythms, with lowest function during the biological night, around 4:00 AM, uncovering a nocturnal exacerbation of asthma usually unnoticed or hidden by the presence of sleep. We also discovered a circadian rhythm in symptom-based rescue bronchodilator use (β2-adrenergic agonist inhaler) whereby inhaler use was four times more likely during the circadian night than day. There were additive influences on asthma from the circadian system plus sleep and other behavioral or environmental effects. Individuals with the lowest average pulmonary function tended to have the largest daily circadian variations and the largest behavioral cycle effects on asthma. When sleep was modeled to occur at night, the summed circadian, behavioral/environmental cycle effects almost perfectly matched the ambulatory data. Thus, the circadian system contributes to the common nocturnal worsening of asthma, implying that internal biological time should be considered for optimal therapy.
Keywords: asthma; bronchodilation; circadian misalignment; circadian rhythms; sleep.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Floyer J., A Treatise of the Asthma (Wilkin, London, 1698).
-
- Dethlefsen U., Repgas R., Ein neues therapieprinzip bei nachtlichen asthma. Klin. Med. (Mosk.) 80, 44–47 (1985).
-
- Turner-Warwick M., Epidemiology of nocturnal asthma. Am. J. Med. 85, 6–8 (1988). - PubMed
-
- Martin R. J., Banks-Schlegel S., Chronobiology of asthma. Am. J. Respir. Crit. Care Med. 158, 1002–1007 (1998). - PubMed
-
- Bagg L. R., Hughes D. T., Diurnal variation in peak expiratory flow in asthmatics. Eur. J. Respir. Dis. 61, 298–302 (1980). - PubMed
