

Cost Analysis of Liver Acquisition Fees Before and After Acuity Circle Policy Implementation
- PMID: 34495291
- PMCID: PMC8427489
- DOI: 10.1001/jamasurg.2021.4406
Cost Analysis of Liver Acquisition Fees Before and After Acuity Circle Policy Implementation
Abstract
Importance: Acuity circles (AC) liver allocation policy was implemented to eliminate donor service area geographic boundaries from liver allocation and to decrease variability in median Model of End-stage Liver Disease (MELD) score at transplant and wait list mortality. However, the broader sharing of organs was also associated with more flights for organ procurements and higher costs associated with the increase in flights.
Objective: To determine whether the costs associated with liver acquisition changed after the implementation of AC allocation.
Design, setting, and participants: This single-center cost comparison study analyzed fees associated with organ acquisition before and after AC allocation implementation. The cost data were collected from a single transplant institute with 2 liver transplant centers, located 30 miles apart, in different donation service areas. Cost, recipient, and transportation data for all cases that included fees associated with liver acquisition from July 1, 2019, to October 31, 2020, were collected.
Exposures: Primary liver offer acceptance with associated organ procurement organization or charter flight fees.
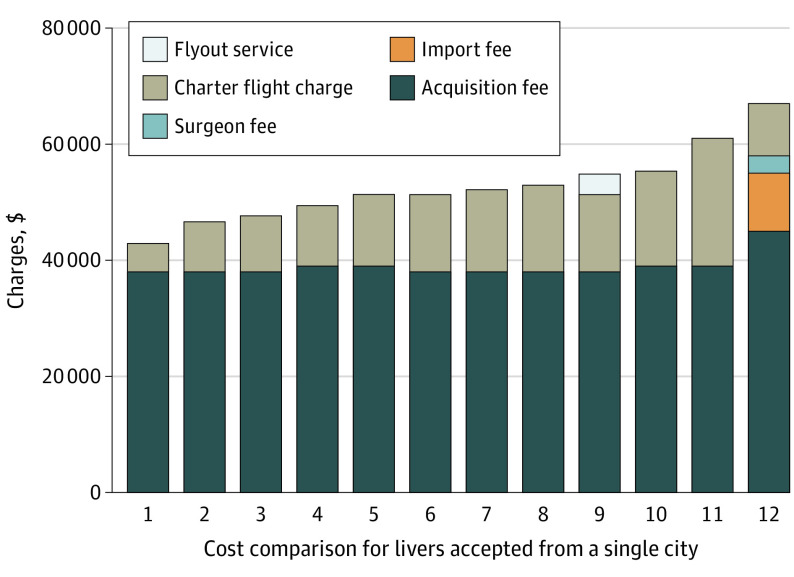
Main outcomes and measures: Specific fees (organ acquisition, surgeon, import, and charter flight fees) and total fees per donor were collected for all accepted liver donors with at least 1 associated fee during the study period.
Results: Of 213 included donors, 171 were used for transplant; 90 of 171 (52.6%) were male, and the median (interquartile range) age of donors was 41.0 (30.0-52.8) years in the pre-AC period and 36.9 (24.0-48.8) years in the post-AC period. There was no significant difference in the post-AC compared with pre-AC period in median (range) MELD score (24 [8-40] vs 25 [6-40]; P = .27) or median (range) match run sequence (15 [1-3951] vs 10 [1-1138]; P = .31), nor in mean (SD) distance traveled (155.83 [157.00] vs 140.54 [144.33] nautical miles; P = .32) or percentage of donors requiring flights (58.5% [69 of 118] vs 56.8% [54 of 95]; P = .82). However, costs increased significantly in the post-AC period: total cost increased 16% per accepted donor (mean [SD] of $52 966 [13 278] vs $45 725 [9300]; P < .001) and 55% per declined donor (mean [SD] of $15 865 [3942] vs $10 217 [4853]; P < .001). Contributing factors included more than 2-fold increases in the proportions of donors incurring import fees (31.4% [37 of 118] vs 12.6% [12 of 95]; P = .002) and surgeon fees (19.5% [23 of 118] vs 9.5% [9 of 95]; P = .05), increased acquisition fees (10% increase; mean [SD] of $43 860 [3266] vs $39 980 [2236]; P < .001), and increased flight expenses (43% increase; mean [SD] of $12 904 [6066] vs $9049 [5140]; P = .002).
Conclusions and relevance: The unintended consequences of implementing broader sharing without addressing organ acquisition fees to account for increased importation between organ procurement organizations must be remedied to contain costs and ensure viability of transplant programs.
Conflict of interest statement
Figures
Comment in
-
Acuity Circles-Higher Cost for Fewer Transplants?JAMA Surg. 2021 Nov 1;156(11):1058. doi: 10.1001/jamasurg.2021.4407. JAMA Surg. 2021. PMID: 34495280 No abstract available.
References
-
- OPTN/UNOS Liver and Intestine Transplantation Committee . Liver and intestine distribution using distance from the donor hospital: briefing paper. Accessed December 21, 2019. https://optn.transplant.hrsa.gov/media/2766/liver_boardreport_201812.pdf
-
- Organ Procurement and Transplant Network . Executive summary of OPTN approval of policies to eliminate the use of DSAs and regions in liver allocation. Accessed December 21, 2019. https://optn.transplant.hrsa.gov/media/2779/board_executivesummary_liver...
-
- US Centers for Medicare & Medicaid Services . Medicare: Provider Reimbursement Manual part 1—Chapter 31, organ acquisition payment policy. Accessed December 18, 2020. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downl...
