

Anti-ADAMTS13 autoantibody profiling in patients with immune-mediated thrombotic thrombocytopenic purpura
- PMID: 34495312
- PMCID: PMC8525240
- DOI: 10.1182/bloodadvances.2020004172
Anti-ADAMTS13 autoantibody profiling in patients with immune-mediated thrombotic thrombocytopenic purpura
Abstract
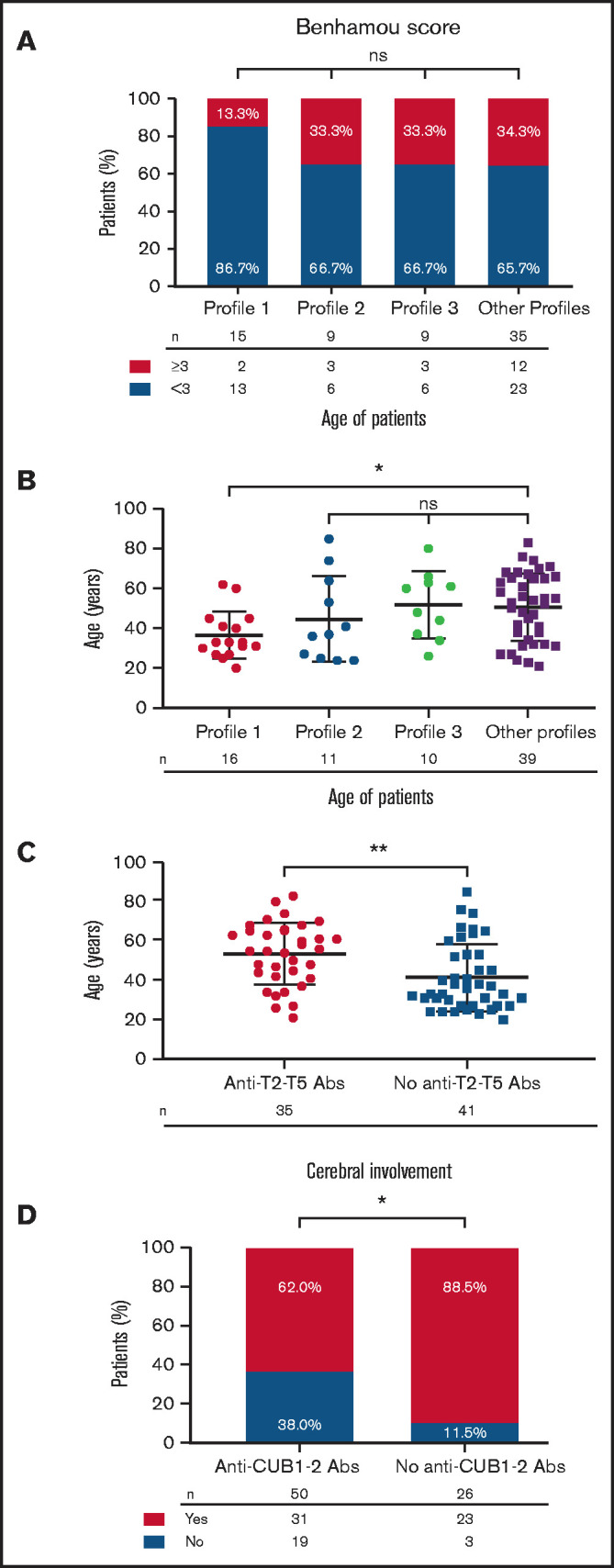
Anti-A Disintegrin and Metalloproteinase with a ThromboSpondin type 1 motif, member 13 (ADAMTS13) autoantibodies cause a severe ADAMTS13 deficiency in immune-mediated thrombotic thrombocytopenic purpura (iTTP). ADAMTS13 consists of a metalloprotease (M), a disintegrin-like (D) domain, 8 thrombospondin type 1 repeats (T1-T8), a cysteine-rich (C), a spacer (S), and 2 CUB domains (CUB1-2). We recently developed a high-throughput epitope mapping assay based on small, nonoverlapping ADAMTS13 fragments (M, DT, CS, T2-T5, T6-T8, CUB1-2). With this assay, we performed a comprehensive epitope mapping using 131 acute-phase samples and for the first time a large group of remission samples (n = 50). Next, samples were stratified according to their immunoprofiles, a field that is largely unexplored in iTTP. Three dominant immunoprofiles were found in acute-phase samples: profile 1: only anti-CS autoantibodies (26.7%); profile 2: both anti-CS and anti-CUB1-2 autoantibodies (12.2%); and profile 3: anti-DT, anti-CS, anti-T2-T5, anti-T6-T8, and anti-CUB1-2 autoantibodies (8.4%). Interestingly, profile 1 was the only dominant immunoprofile in remission samples (52.0%). Clinical data were available for a relatively small number of patients with acute iTTP (>68), and no correlation was found between immunoprofiles and disease severity. Nevertheless, profile 1 was linked with younger and anti-T2-T5 autoantibodies with older age and the absence of anti-CUB1-2 autoantibodies with cerebral involvement. In conclusion, identifying acute phase and remission immunoprofiles in iTTP revealed that anti-CS autoantibodies seem to persist or reappear during remission providing further support for the clinical development of a targeted anti-CS autoantibody therapy. A large cohort study with acute iTTP samples will validate possible links between immunoprofiles or anti-domain autoantibodies and clinical data.
© 2021 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: B.L. is a member of the Advisory board of Ablynx-Sanofi for caplacizumab, holds a patent on von Willebrand factor-cleaving protease, and has received lecture fees or congress travel support by Siemens, Roche, Ablynx-Sanofi, Bayer, and Alexion. F.P.P.C. is a member of the Clinical Advisory Board for Alexion, Ablynx-Sanofi, Shire-Takeda, and Octapharma. A.V. is a member of the Clinical Advisory Board for Ablynx-Sanofi and Shire-Takeda. K.V. is a member of the advisory board of Shire-Takeda and Ablynx-Sanofi. The remaining authors declare no competing financial interests.
Figures




References
-
- Kremer Hovinga JA, Coppo P, Lämmle B, Moake JL, Miyata T, Vanhoorelbeke K.. Thrombotic thrombocytopenic purpura. Nat Rev Dis Primers. 2017;3:17020. - PubMed
-
- Tersteeg C, Verhenne S, Roose E, et al. . ADAMTS13 and anti-ADAMTS13 autoantibodies in thrombotic thrombocytopenic purpura - current perspectives and new treatment strategies. Expert Rev Hematol. 2016;9(2):209-221. - PubMed
-
- Zheng X, Chung D, Takayama TK, Majerus EM, Sadler JE, Fujikawa K.. Structure of von Willebrand factor-cleaving protease (ADAMTS13), a metalloprotease involved in thrombotic thrombocytopenic purpura. J Biol Chem. 2001;276(44):41059-41063. - PubMed
-
- Rieger M, Ferrari S, Kremer Hovinga JA, et al. . Relation between ADAMTS13 activity and ADAMTS13 antigen levels in healthy donors and patients with thrombotic microangiopathies (TMA). Thromb Haemost. 2006;95(2):212-220. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
