

Current treatment of IgA nephropathy
- PMID: 34495361
- PMCID: PMC8551131
- DOI: 10.1007/s00281-021-00888-3
Current treatment of IgA nephropathy
Abstract
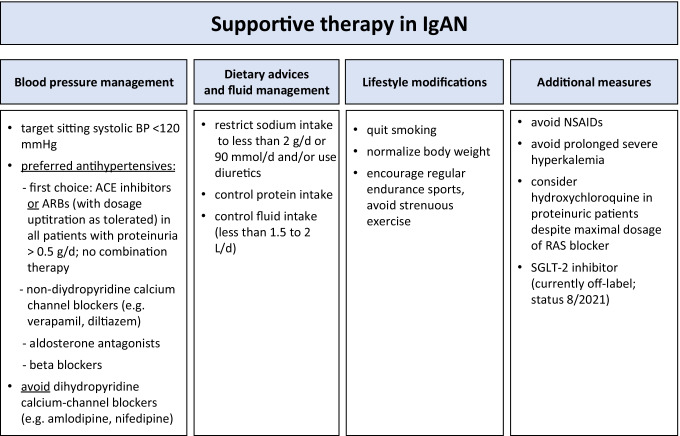
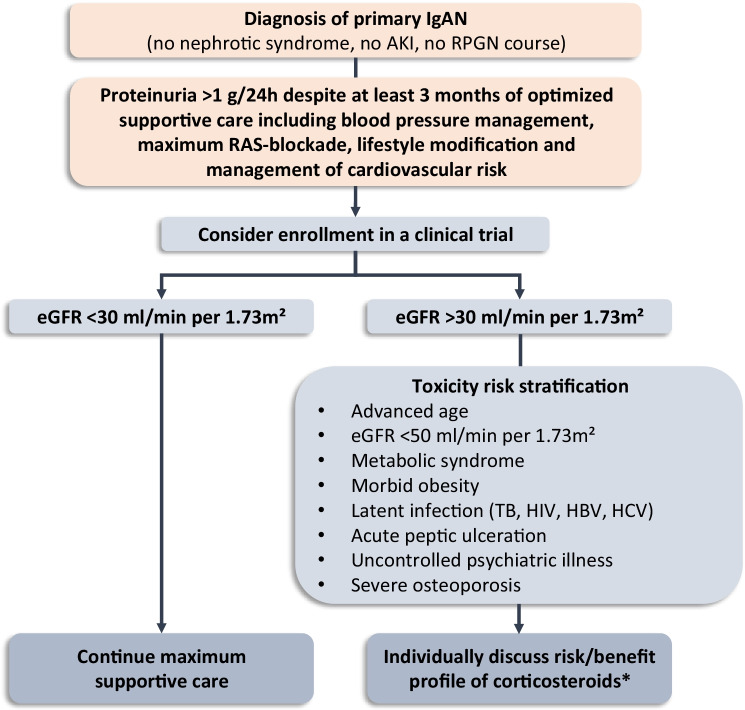
IgA nephropathy (IgAN) is the most common type of glomerulonephritis in Asia and the Western world. In most patients, it follows an asymptomatic to oligosymptomatic course and GFR loss, if any, is slow. The mainstay of therapy therefore is optimized supportive care, i.e., measures that lower blood pressure, reduce proteinuria, minimize lifestyle risk factors, and otherwise help to reduce non-specific insults to the kidneys. The value of immunosuppression has become controversial and if at all, systemic high-dose corticosteroid therapy should be considered for a few months taking into account patient characteristics that would caution against or preclude such therapy. In addition, adverse events related to corticosteroid therapy markedly increase as GFR declines. Beyond corticosteroids, there is little evidence that any additional immunosuppression is helpful, with the exception of mycophenolate mofetil in patients of Asian descent. A considerable number of clinical trials ranging from enteric coated budesonide to blockade of B-cell function to complement inhibitors are currently ongoing and will hopefully allow a more targeted therapy of high-risk patients with progressive IgAN in the future.
Keywords: Complement; Glucocorticoids; IgA nephropathy; Mesangioproliferative glomerulonephritis; Supportive therapy.
© 2021. The Author(s).
Conflict of interest statement
J. Floege has received honoraria from Calliditas, Omeros, and Travere. S. Tang has received honoraria from AstraZeneca, Sanofi, and Novartis. T. Rauen has no conflicts of interest to declare.
Figures

References
-
- Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med. 2013;368:2402–2414. - PubMed
-
- Moreno JA, Martin-Cleary C, Gutierrez E, Toldos O, Blanco-Colio LM, Praga M, Ortiz A, Egido J. AKI associated with macroscopic glomerular hematuria: clinical and pathophysiologic consequences. Clinical journal of the American Society of Nephrology : CJASN. 2012;7:175–184. - PubMed
-
- Roccatello D, Ferro M, Coppo R, Mazzucco G, Quattrocchio G, Piccoli G. Treatment of rapidly progressive IgA nephropathy. Contrib Nephrol. 1995;111:177–82. - PubMed
-
- Stefanski A, Schmidt KG, Waldherr R, Ritz E. Early increase in blood pressure and diastolic left ventricular malfunction in patients with glomerulonephritis. Kidney Int. 1996;50:1321–1326. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
