

Pharmacological Treatments for Borderline Personality Disorder: A Systematic Review and Meta-Analysis
- PMID: 34495494
- PMCID: PMC8478737
- DOI: 10.1007/s40263-021-00855-4
Pharmacological Treatments for Borderline Personality Disorder: A Systematic Review and Meta-Analysis
Abstract
Background: Borderline personality disorder (BPD) is a debilitating psychiatric disorder that affects 0.4-3.9% of the population in Western countries. Currently, no medications have been approved by regulatory agencies for the treatment of BPD. Nevertheless, up to 96% of patients with BPD receive at least one psychotropic medication.
Objectives: The objective of this systematic review was to assess the general efficacy and the comparative effectiveness of different pharmacological treatments for BPD patients.
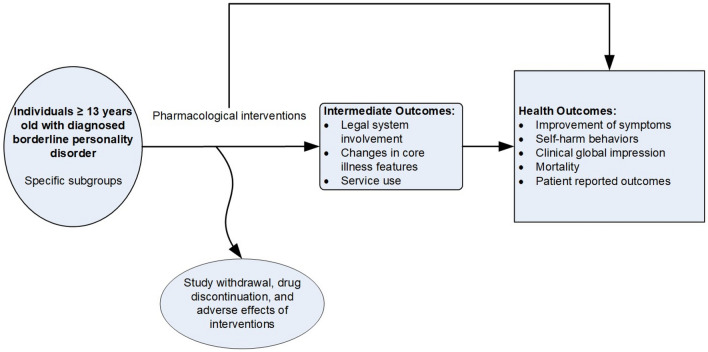
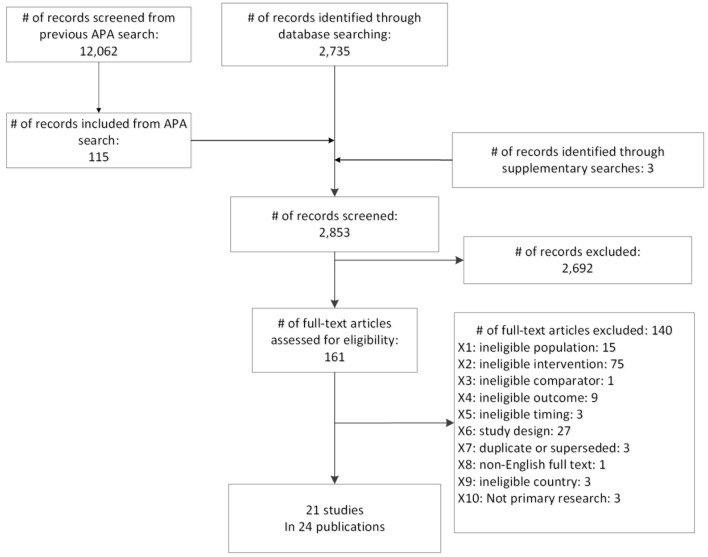
Methods: We conducted systematic literature searches limited to English language in MEDLINE, EMBASE, the Cochrane Library, and PsycINFO up to April 6, 2021, and searched reference lists of pertinent articles and reviews. Inclusion criteria were (i) patients 13 years or older with a diagnosis of BPD, (ii) treatment with anticonvulsive medications, antidepressants, antipsychotic medications, benzodiazepines, melatonin, opioid agonists or antagonists, or sedative or hypnotic medications for at least 8 weeks, (iii) comparison with placebo or an eligible medication, (iv) assessment of health-relevant outcomes, (v) randomized or non-randomized trials or controlled observational studies. Two investigators independently screened abstracts and full-text articles and graded the certainty of evidence based on the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach. For meta-analyses, we used restricted maximum likelihood random effects models to estimate pooled effects.
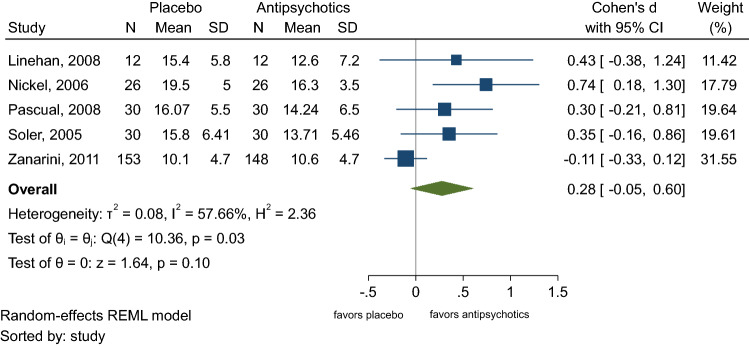
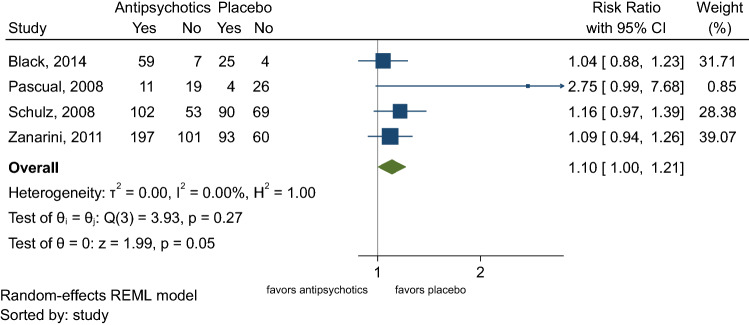
Results: Of 12,062 unique records, we included 21 randomized controlled trials (RCTs) with data on 1768 participants. Nineteen RCTs compared pharmacotherapies with placebo; two RCTs assessed active treatments head-to-head. Out of 87 medications in use in clinical practice, we found studies on just nine. Overall, the evidence indicates that the efficacy of pharmacotherapies for the treatment of BPD is limited. Second-generation antipsychotics, anticonvulsants, and antidepressants were not able to consistently reduce the severity of BPD. Low-certainty evidence indicates that anticonvulsants can improve specific symptoms associated with BPD such as anger, aggression, and affective lability but the evidence is mostly limited to single studies. Second-generation antipsychotics had little effect on the severity of specific BPD symptoms, but they improved general psychiatric symptoms in patients with BPD.
Conclusions: Despite the common use of pharmacotherapies for patients with BPD, the available evidence does not support the efficacy of pharmacotherapies alone to reduce the severity of BPD.
Registration: PROSPERO registration number, CRD42020194098.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no potential conflicts of interest.
Figures
Comment in
-
Comment on "Pharmacological Treatments for Borderline Personality Disorder: A Systematic Review and Meta-Analysis".CNS Drugs. 2021 Dec;35(12):1333-1334. doi: 10.1007/s40263-021-00872-3. Epub 2021 Nov 7. CNS Drugs. 2021. PMID: 34743293 No abstract available.
-
Authors' Reply to Pereira Ribeiro et al.: Comment on "Pharmacological Treatments for Borderline Personality Disorder: A Systematic Review and Meta‑Analysis".CNS Drugs. 2021 Dec;35(12):1335-1336. doi: 10.1007/s40263-021-00873-2. Epub 2021 Nov 7. CNS Drugs. 2021. PMID: 34743294 No abstract available.
References
-
- Leichsenring F, et al. Borderline personality disorder. Lancet. 2011;377(9759):74–84. - PubMed
-
- Oldham JM. Borderline personality disorder and suicidality. Am J Psychiatry. 2006;163(1):20–26. - PubMed
-
- American Psychiatric Association, Diagnostic and statistical manual of mental disorders (DSM-5®). Washington D.C.: American Psychiatric Publishing; 2013. p. 645, 663–6.
-
- World Health Organization (WHO). The ICD-10 classification of mental and behavioural disorders. World Health Organization. 1993 April 3, 2021. https://www.who.int/classifications/icd/en/bluebook.pdf.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
