

A Modeling Study of a Patient-specific Safe Zone for THA: Calculation, Validation, and Key Factors Based on Standing and Sitting Sagittal Pelvic Tilt
- PMID: 34495893
- PMCID: PMC8673979
- DOI: 10.1097/CORR.0000000000001923
A Modeling Study of a Patient-specific Safe Zone for THA: Calculation, Validation, and Key Factors Based on Standing and Sitting Sagittal Pelvic Tilt
Abstract
Background: Lumbar-pelvic stiffness and sagittal imbalance have been reported to increase the risk of dislocation and wear after THA. One potential way to approach this concern is by identifying patient-specific safe zones for THA components based on the standing and sitting sagittal pelvic tilt. However, there is no algorithm to integrate the standing and sitting pelvic tilt into the surgical plan of component orientations.
Questions/purposes: We established a new mathematical algorithm for determining a patient-specific safe zone for THA by integrating the impingement-free ROM requirements of standing and sitting while preventing edge loading while standing. We aimed to determine (1) the accuracy of this new method for predicting the impingement-free ROM for a given component orientation, (2) the sensitivity and specificity of detecting an impingement-free acetabular cup position for standing and sitting, and (3) the influences of key factors including pelvic tilt while standing and pelvic tilt while sitting and implant parameters on patient-specific safe zones.
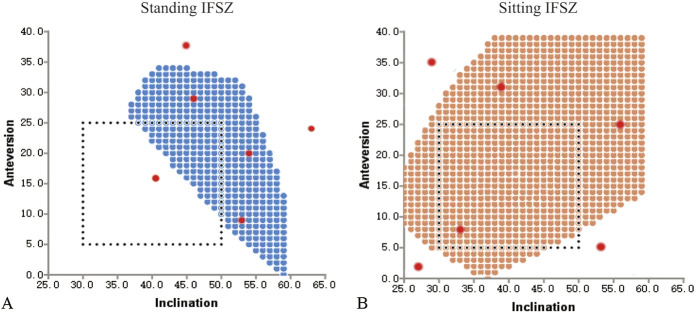
Methods: A strategy for calculating the intersection of standing and sitting impingement-free safe zones and the zone of a standing radiographic inclination of ≤ 45° was used to develop patient-specific safe zones. We conducted a computer simulation study including the pelvis and THA prosthesis to answer the three study questions. We enrolled 10 patients who underwent robot-assisted THA for avascular necrosis of the femoral head (mean age 49 ± 19 years; five were women) from October 2019 to December 2019. We used a prosthesis model with a conical stem neck and a non-hooded liner, with the femoral head diameter ranging between 28 mm and 40 mm, and the corresponding head-neck ratio ranging between 2.33 and 3.33. We tested 1680 movements for the accuracy of impingement-free ROM (Question 1), and 80 marginal points and 120 non-marginal points of the comprehensive impingement-free safe zone, which combines the standing and sitting postures (Question 2). For Question 3, we explored the influences of standing and sitting pelvic tilt, femoral head diameter, and ROM criteria on the size of the patient-specific safe zone.
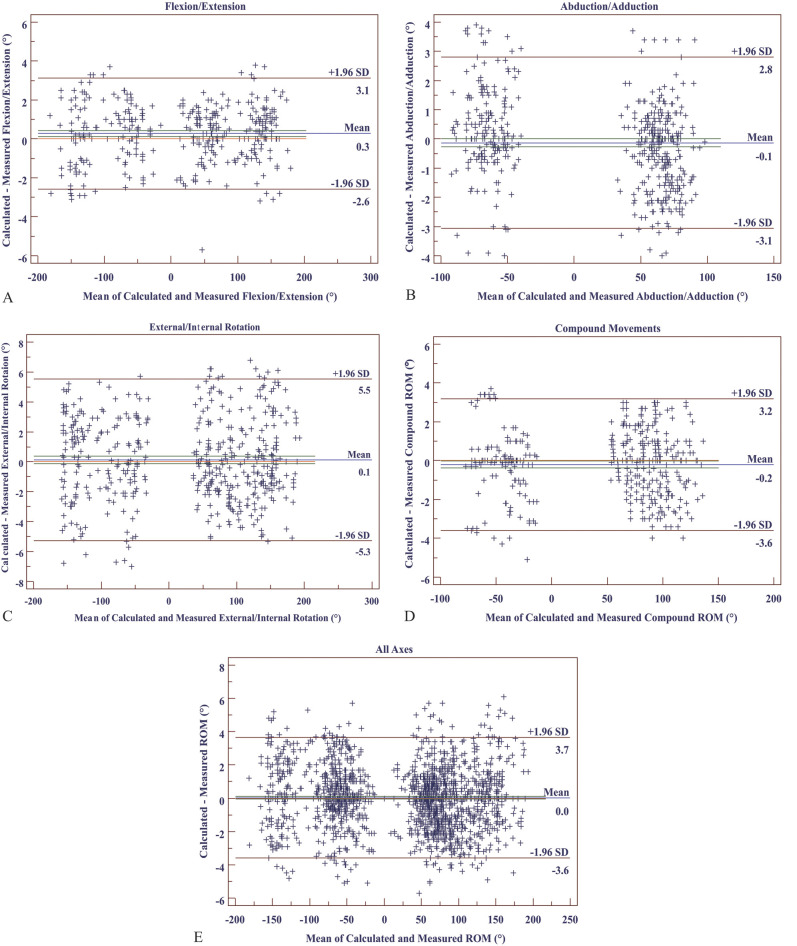
Results: With the simulation method as a reference for detecting impingement, the mean absolute error (arithmetic mean of all the absolute errors) of the calculated impingement-free ROM was 1.4° ± 2.3°, and the limit of agreement of errors was between -3.6° and 3.7°. The sensitivity of detecting a safe cup orientation within the comprehensive impingement-free safe zone for a given ROM criterion was 98.9% (95% CI 93.6% to 99.9%), and specificity was 97.1% (95% CI 91.0% to 99.2%). There were no impingement-free safe zones for 29% (pelvic tilt combinations without an impingement-free safe zone and all tested combinations) and no patient-specific safe zones for 46% (pelvic tilt combinations without a patient-specific safe zone and all tested combinations) of the tested combinations of standing and sitting pelvic tilt. The patient-specific safe zone was sensitive to changes in standing and sitting pelvic tilt, femoral head diameter, stem version, and ROM criteria. Stem anteversions beyond 10° to 20° dramatically reduced the size of the patient-specific safe zone to 0 within a change of 10° to 20°.
Conclusion: The patient-specific safe zone algorithm can be an accurate method for determining the optimal orientation for acetabular cups and femoral stems in THA. The patient-specific safe zone is sensitive to changes in standing and sitting pelvic tilt, stem version, ROM criteria, and the femoral head diameter. A narrow zone of 10° to 20° for stem anteversion is recommended to maximize the size of the patient-specific safe zone.
Clinical relevance: This study suggests the potential of a mathematical algorithm to optimize the orientation of THA components and illustrates how key parameters affect the patient-specific safe zone.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures









Comment in
-
CORR Insights®: A Modeling Study of a Patient-specific Safe Zone for THA: Calculation, Validation, and Key Factors Based on Standing and Sitting Sagittal Pelvic Tilt.Clin Orthop Relat Res. 2022 Jan 1;480(1):206-208. doi: 10.1097/CORR.0000000000001976. Clin Orthop Relat Res. 2022. PMID: 34525000 Free PMC article. No abstract available.
References
-
- Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Biomechanics of large femoral heads: what they do and don't do. Clin Orthop Relat Res. 2004;429:102-107. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
