

Effectiveness of seasonal malaria chemoprevention (SMC) treatments when SMC is implemented at scale: Case-control studies in 5 countries
- PMID: 34495978
- PMCID: PMC8457484
- DOI: 10.1371/journal.pmed.1003727
Effectiveness of seasonal malaria chemoprevention (SMC) treatments when SMC is implemented at scale: Case-control studies in 5 countries
Abstract
Background: Seasonal malaria chemoprevention (SMC) has shown high protective efficacy against clinical malaria and severe malaria in a series of clinical trials. We evaluated the effectiveness of SMC treatments against clinical malaria when delivered at scale through national malaria control programmes in 2015 and 2016.
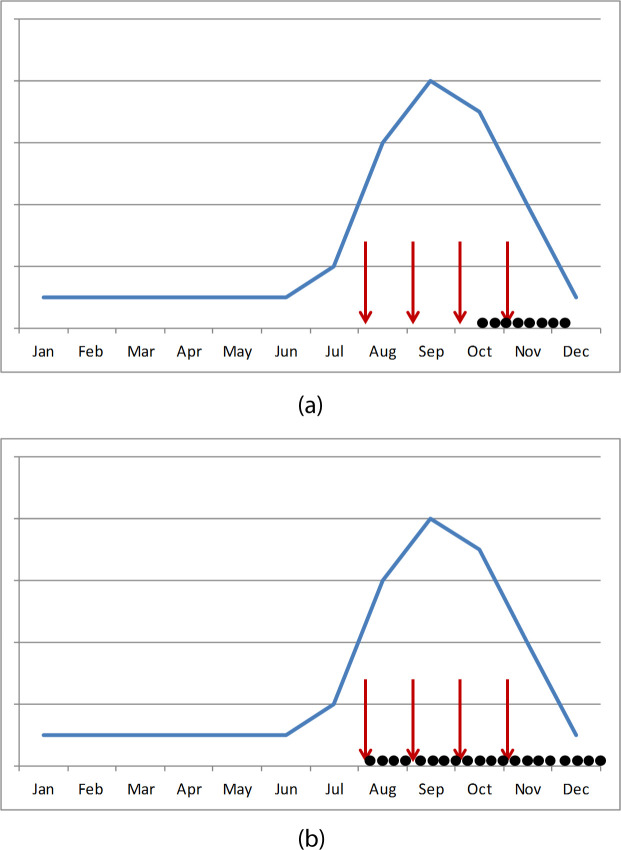
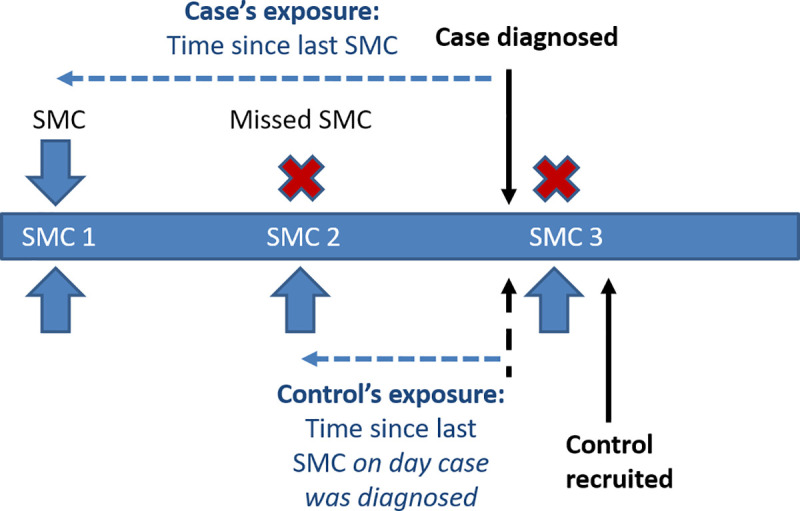
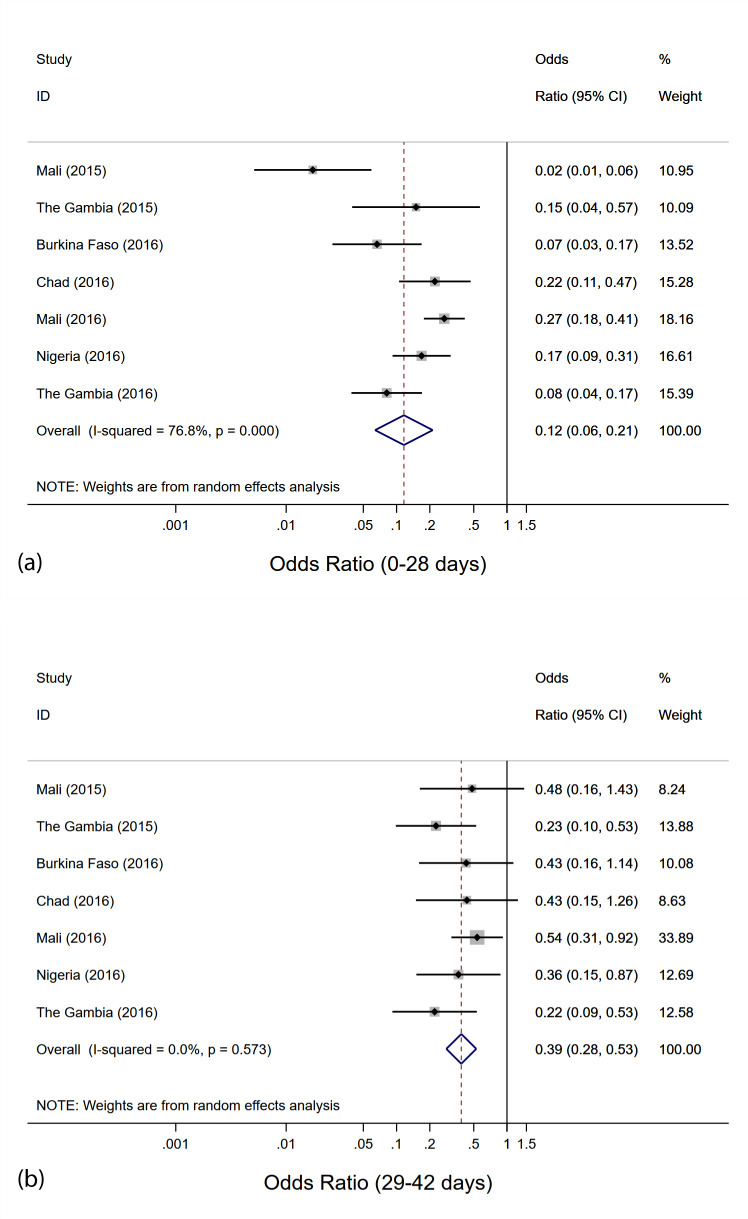
Methods and findings: Case-control studies were carried out in Mali and The Gambia in 2015, and in Burkina Faso, Chad, Mali, Nigeria, and The Gambia in 2016. Children aged 3-59 months presenting at selected health facilities with microscopically confirmed clinical malaria were recruited as cases. Two controls per case were recruited concurrently (on or shortly after the day the case was detected) from the neighbourhood in which the case lived. The primary exposure was the time since the most recent course of SMC treatment, determined from SMC recipient cards, caregiver recall, and administrative records. Conditional logistic regression was used to estimate the odds ratio (OR) associated with receipt of SMC within the previous 28 days, and SMC 29 to 42 days ago, compared with no SMC in the past 42 days. These ORs, which are equivalent to incidence rate ratios, were used to calculate the percentage reduction in clinical malaria incidence in the corresponding time periods. Results from individual countries were pooled in a random-effects meta-analysis. In total, 2,126 cases and 4,252 controls were included in the analysis. Across the 7 studies, the mean age ranged from 1.7 to 2.4 years and from 2.1 to 2.8 years among controls and cases, respectively; 42.2%-50.9% and 38.9%-46.9% of controls and cases, respectively, were male. In all 7 individual case-control studies, a high degree of personal protection from SMC against clinical malaria was observed, ranging from 73% in Mali in 2016 to 98% in Mali in 2015. The overall OR for SMC within 28 days was 0.12 (95% CI: 0.06, 0.21; p < 0.001), indicating a protective effectiveness of 88% (95% CI: 79%, 94%). Effectiveness against clinical malaria for SMC 29-42 days ago was 61% (95% CI: 47%, 72%). Similar results were obtained when the analysis was restricted to cases with parasite density in excess of 5,000 parasites per microlitre: Protective effectiveness 90% (95% CI: 79%, 96%; P<0.001), and 59% (95% CI: 34%, 74%; P<0.001) for SMC 0-28 days and 29-42 days ago, respectively. Potential limitations include the possibility of residual confounding due to an association between exposure to malaria and access to SMC, or differences in access to SMC between patients attending a clinic and community controls; however, neighbourhood matching of cases and controls, and covariate adjustment, attempted to control for these aspects, and the observed decline in protection over time, consistent with expected trends, argues against a major bias from these sources.
Conclusions: SMC administered as part of routine national malaria control activities provided a very high level of personal protection against clinical malaria over 28 days post-treatment, similar to the efficacy observed in clinical trials. The case-control design used in this study can be used at intervals to ensure SMC treatments remain effective.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. WHO policy recommendation: seasonal malaria chemoprevention (SMC) for Plasmodium falciparum malaria control in highly seasonal transmission areas of the Sahel sub-region in Africa. Geneva: World Health Organization; 2012. [cited 2021 Aug 26]. Available from: https://www.who.int/malaria/mpac/feb2012/smc_policy_recommendation.pdf.
-
- London School of Hygiene & Tropical Medicine. OPT-SMC: SMC in 2020. London: London School of Hygiene & Tropical Medicine; 2021. [cited 2021 Aug 27]. Available from: https://www.lshtm.ac.uk/research/centres-projects-groups/opt-smc#smc-in-....
-
- Griffin JT, Cairns M, Ghani AC, Roper C, Schellenberg D, Carneiro I, et al. Protective efficacy of intermittent preventive treatment of malaria in infants (IPTi) using sulfadoxine-pyrimethamine and parasite resistance. PLoS ONE. 2010;5(9):e12618. doi: 10.1371/journal.pone.0012618 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
