

Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity
- PMID: 34496632
- PMCID: PMC8478888
- DOI: 10.1161/CIRCULATIONAHA.120.049755
Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity
Erratum in
-
Correction to: Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity.Circulation. 2022 Jun 7;145(23):e1072. doi: 10.1161/CIR.0000000000001080. Epub 2022 May 20. Circulation. 2022. PMID: 35593721 No abstract available.
-
Correction to: Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity.Circulation. 2022 Jul 5;146(1):e3. doi: 10.1161/CIR.0000000000001084. Epub 2022 Jun 14. Circulation. 2022. PMID: 35700338 No abstract available.
Abstract
Background: The ISCHEMIA trial (International Study of Comparative Health Effectiveness With Medical and Invasive Approaches) postulated that patients with stable coronary artery disease (CAD) and moderate or severe ischemia would benefit from revascularization. We investigated the relationship between severity of CAD and ischemia and trial outcomes, overall and by management strategy.
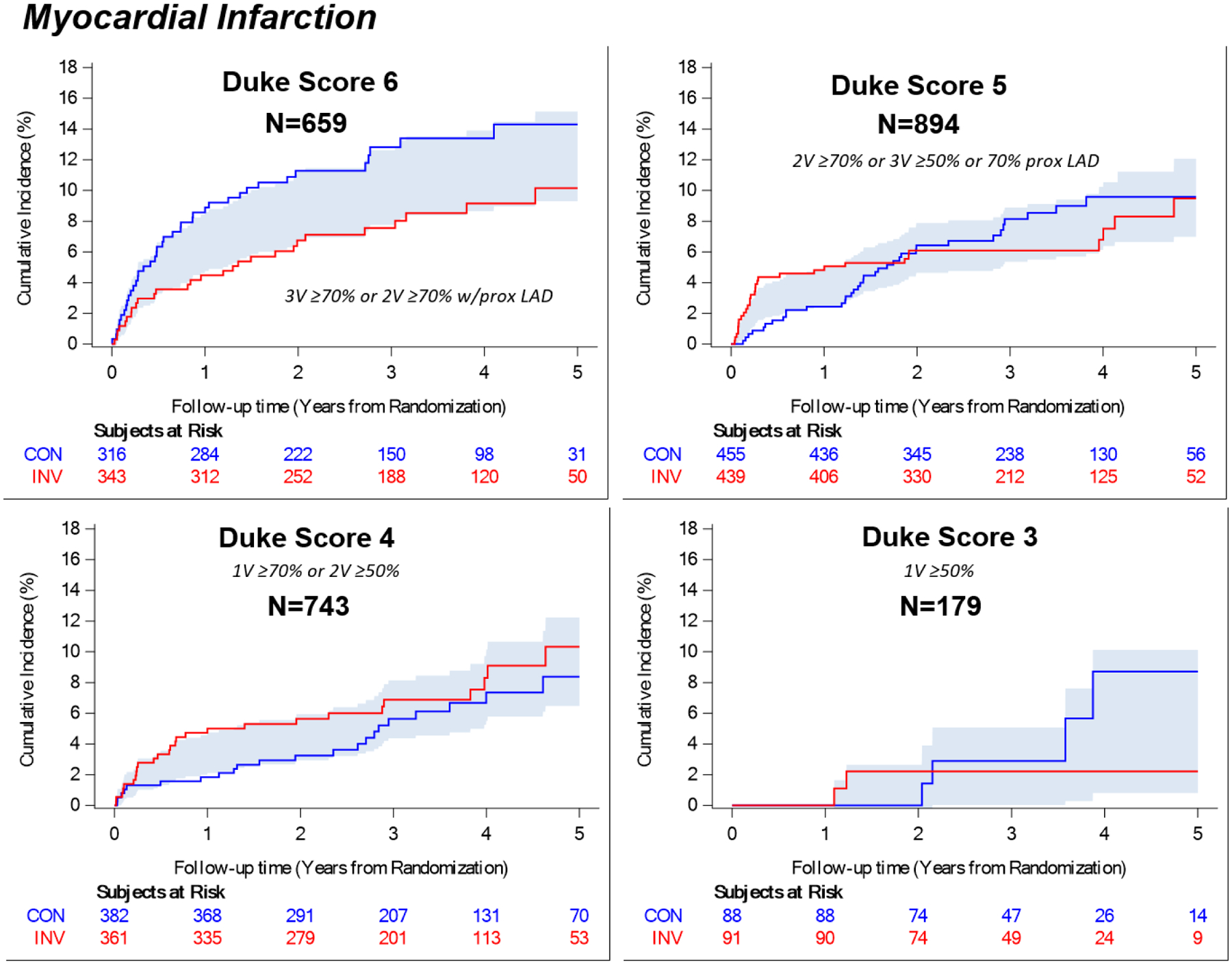
Methods: In total, 5179 patients with moderate or severe ischemia were randomized to an initial invasive or conservative management strategy. Blinded, core laboratory-interpreted coronary computed tomographic angiography was used to assess anatomic eligibility for randomization. Extent and severity of CAD were classified with the modified Duke Prognostic Index (n=2475, 48%). Ischemia severity was interpreted by independent core laboratories (nuclear, echocardiography, magnetic resonance imaging, exercise tolerance testing, n=5105, 99%). We compared 4-year event rates across subgroups defined by severity of ischemia and CAD. The primary end point for this analysis was all-cause mortality. Secondary end points were myocardial infarction (MI), cardiovascular death or MI, and the trial primary end point (cardiovascular death, MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest).
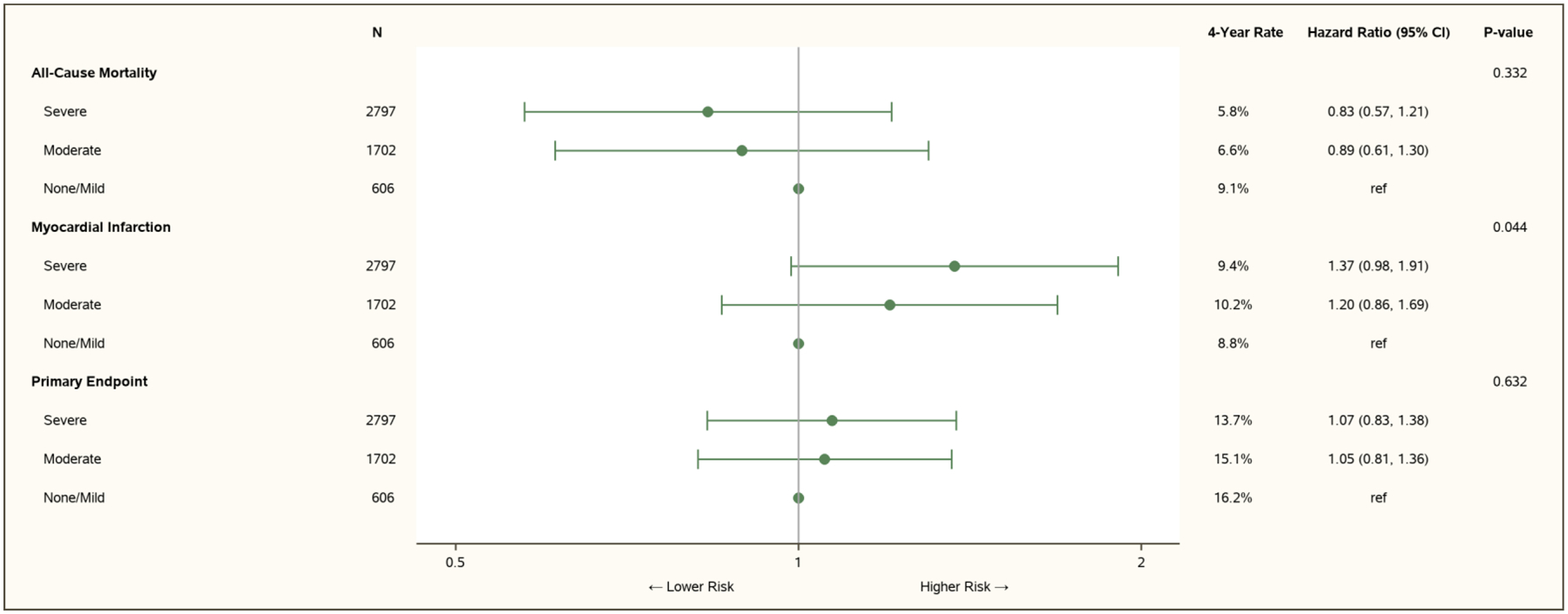
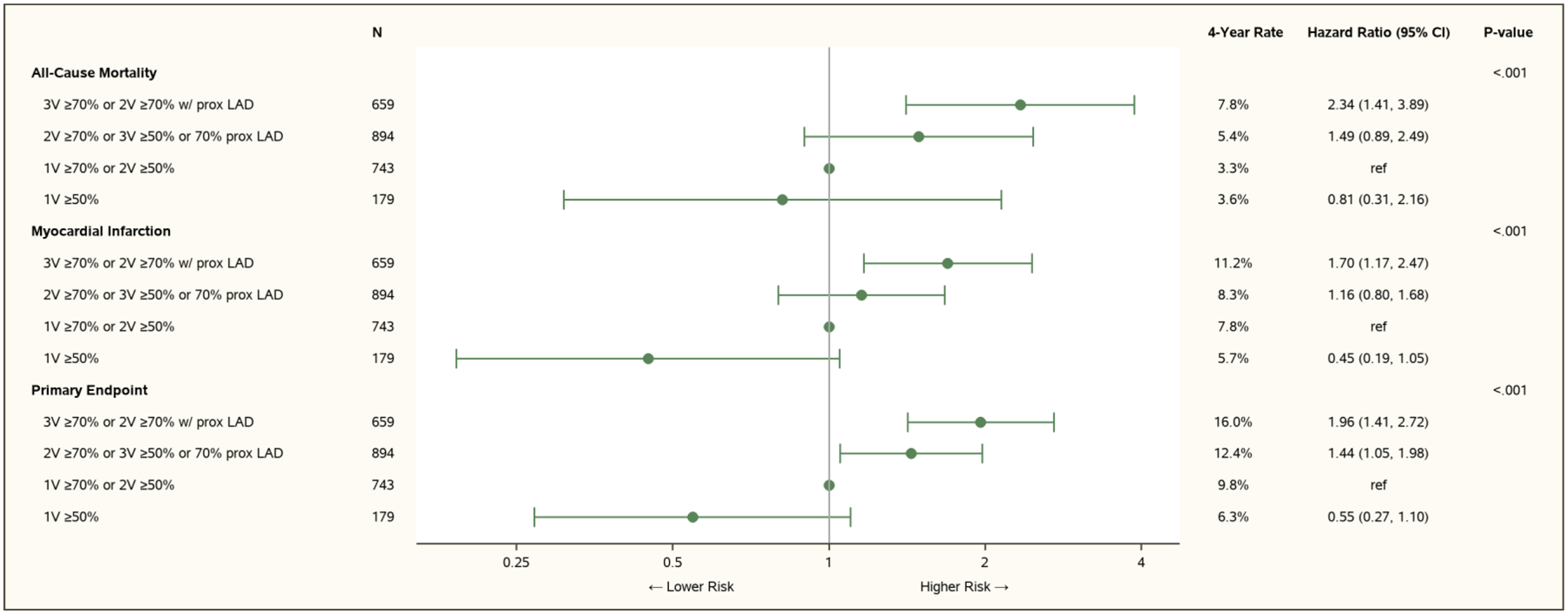
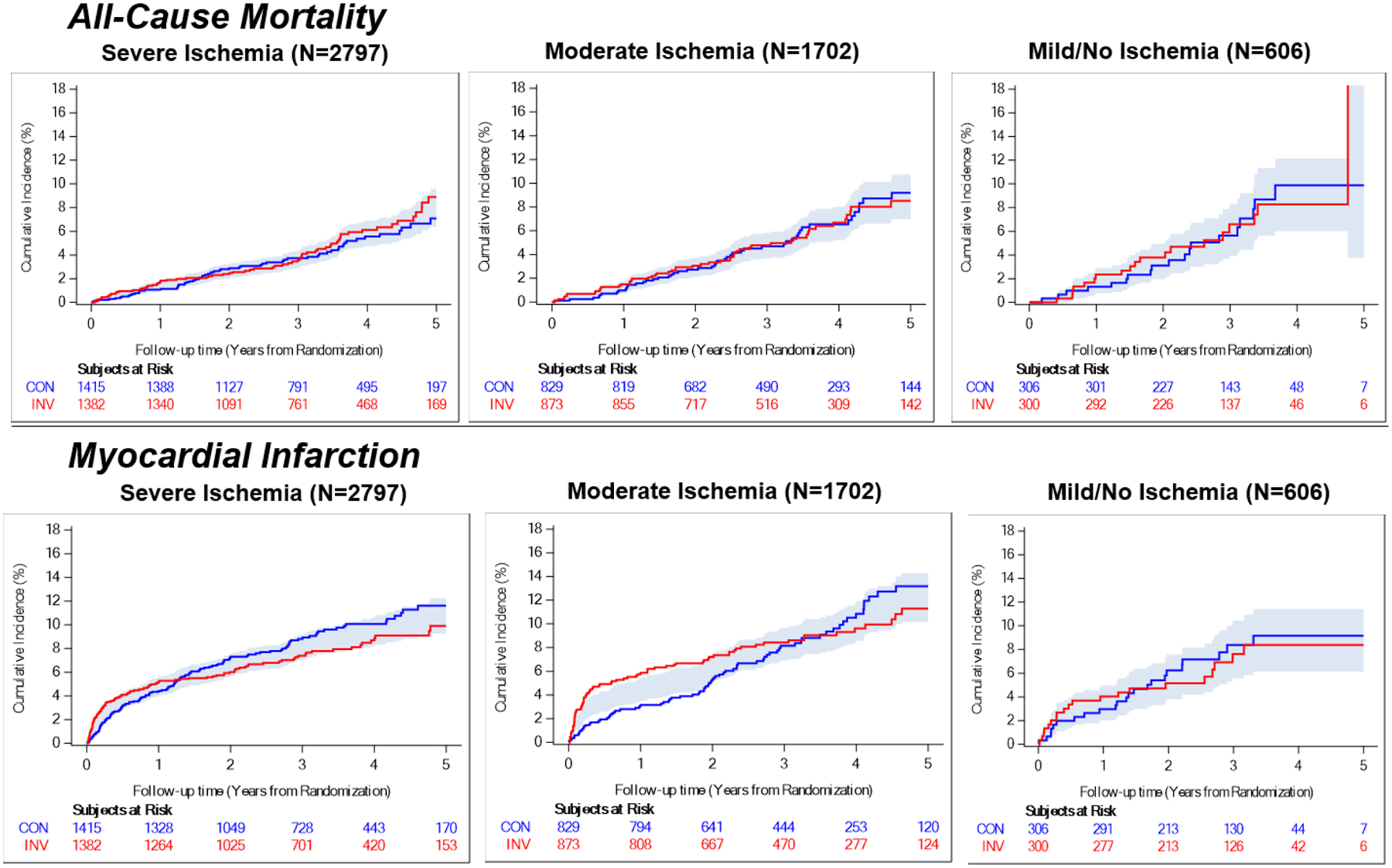
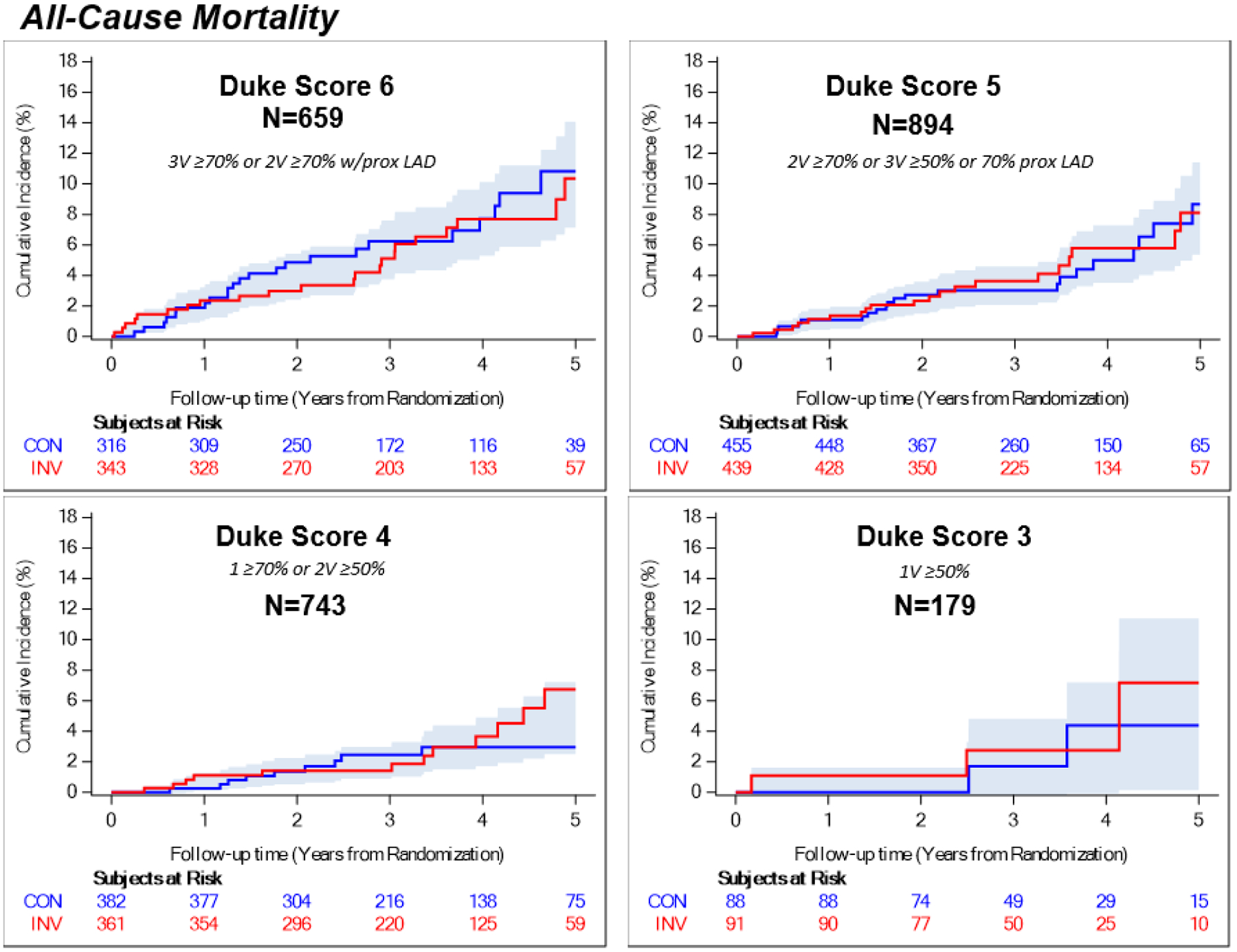
Results: Relative to mild/no ischemia, neither moderate ischemia nor severe ischemia was associated with increased mortality (moderate ischemia hazard ratio [HR], 0.89 [95% CI, 0.61-1.30]; severe ischemia HR, 0.83 [95% CI, 0.57-1.21]; P=0.33). Nonfatal MI rates increased with worsening ischemia severity (HR for moderate ischemia, 1.20 [95% CI, 0.86-1.69] versus mild/no ischemia; HR for severe ischemia, 1.37 [95% CI, 0.98-1.91]; P=0.04 for trend, P=NS after adjustment for CAD). Increasing CAD severity was associated with death (HR, 2.72 [95% CI, 1.06-6.98]) and MI (HR, 3.78 [95% CI, 1.63-8.78]) for the most versus least severe CAD subgroup. Ischemia severity did not identify a subgroup with treatment benefit on mortality, MI, the trial primary end point, or cardiovascular death or MI. In the most severe CAD subgroup (n=659), the 4-year rate of cardiovascular death or MI was lower in the invasive strategy group (difference, 6.3% [95% CI, 0.2%-12.4%]), but 4-year all-cause mortality was similar.
Conclusions: Ischemia severity was not associated with increased risk after adjustment for CAD severity. More severe CAD was associated with increased risk. Invasive management did not lower all-cause mortality at 4 years in any ischemia or CAD subgroup. Registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT01471522.
Keywords: coronary artery bypass; coronary artery disease; ischemia; myocardial revascularization; percutaneous coronary intervention.
Figures
References
-
- Maron DJ, Hochman JS, O’Brien SM, Reynolds HR, Boden WE, Stone GW, Bangalore S, Spertus JA, Mark DB, Alexander KP, et al. International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial: Rationale and design. American Heart Journal. 2018;201:124–135. - PMC - PubMed
-
- Hachamovitch R, Hayes SW, Friedman JD, Cohen I and Berman DS. Comparison of the Short-Term Survival Benefit Associated With Revascularization Compared With Medical Therapy in Patients With No Prior Coronary Artery Disease Undergoing Stress Myocardial Perfusion Single Photon Emission Computed Tomography. 2003;107:2900–2907. - PubMed
-
- Yao SS, Bangalore S and Chaudhry FA. Prognostic implications of stress echocardiography and impact on patient outcomes: an effective gatekeeper for coronary angiography and revascularization. J Am Soc Echocardiogr. 2010;23:832–9. - PubMed
-
- Mancini GBJ, Hartigan PM, Shaw LJ, Berman DS, Hayes SW, Bates ER, Maron DJ, Teo K, Sedlis SP, Chaitman BR, et al. Predicting outcome in the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation): coronary anatomy versus ischemia. JACC Cardiovascular interventions. 2014;7:195–201. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
