

Association of medical male circumcision and sexually transmitted infections in a population-based study using targeted maximum likelihood estimation
- PMID: 34496810
- PMCID: PMC8425067
- DOI: 10.1186/s12889-021-11705-9
Association of medical male circumcision and sexually transmitted infections in a population-based study using targeted maximum likelihood estimation
Abstract
Background: Epidemiological theory and many empirical studies support the hypothesis that there is a protective effect of male circumcision against some sexually transmitted infections (STIs). However, there is a paucity of randomized control trials (RCTs) to test this hypothesis in the South African population. Due to the infeasibility of conducting RCTs, estimating marginal or average treatment effects with observational data increases interest. Using targeted maximum likelihood estimation (TMLE), a doubly robust estimation technique, we aim to provide evidence of an association between medical male circumcision (MMC) and two STI outcomes.
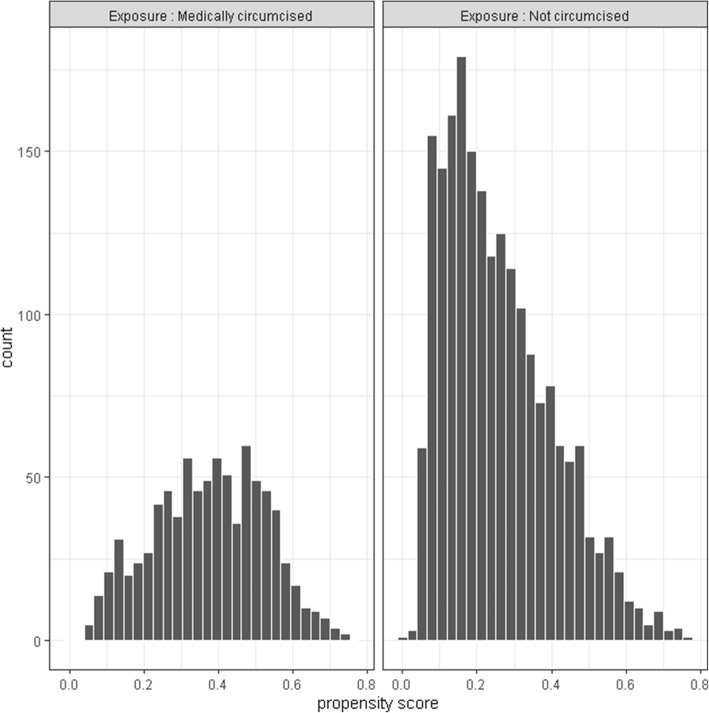
Methods: HIV and HSV-2 status were the two primary outcomes for this study. We investigated the associations between MMC and these STI outcomes, using cross-sectional data from the HIV Incidence Provincial Surveillance System (HIPSS) study in KwaZulu-Natal, South Africa. HIV antibodies were tested from the blood samples collected in the study. For HSV-2, serum samples were tested for HSV-2 antibodies via an ELISA-based anti-HSV-2 IgG. We estimated marginal prevalence ratios (PR) using TMLE and compared estimates with those from propensity score full matching (PSFM) and inverse probability of treatment weighting (IPTW).
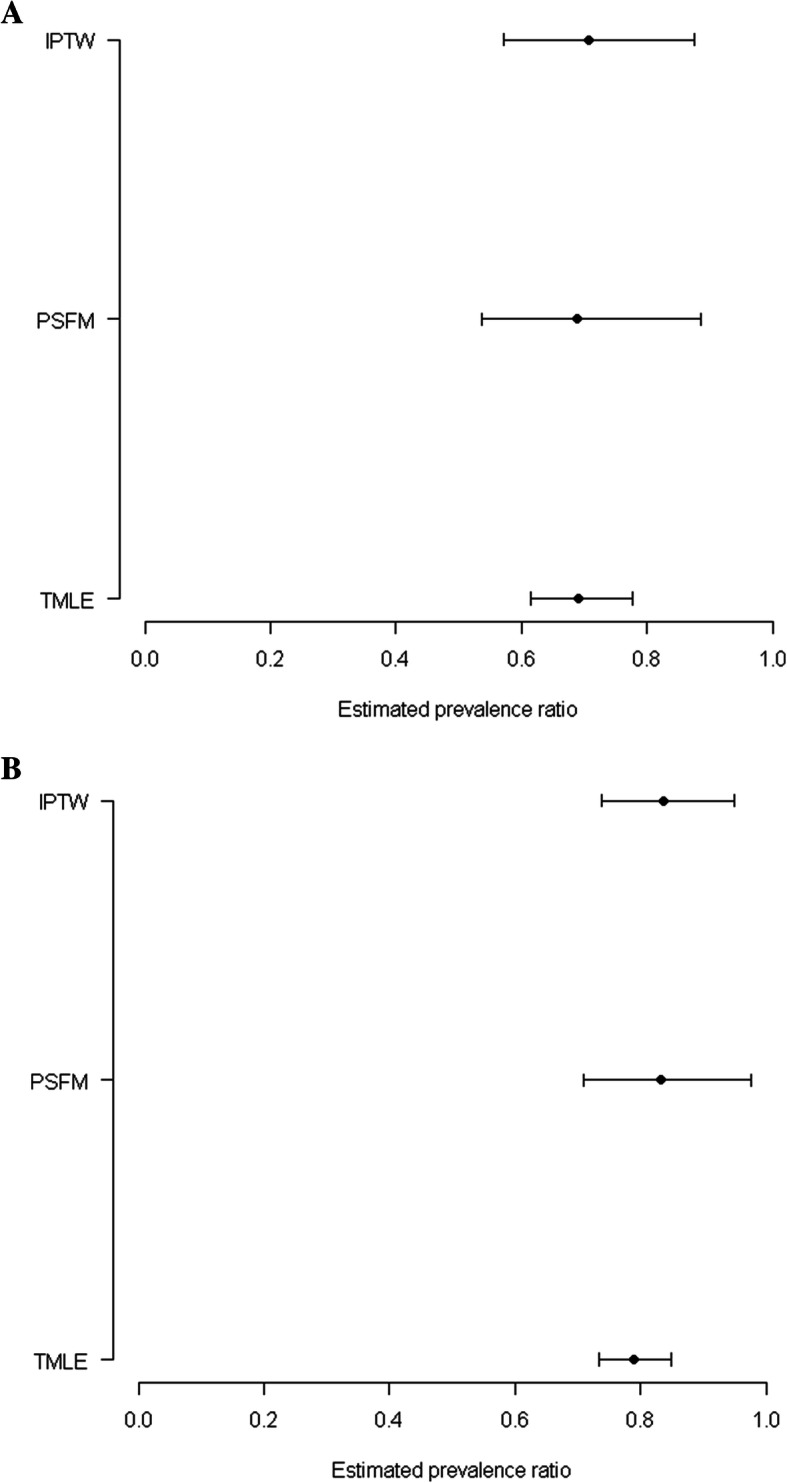
Results: From a total 2850 male participants included in the analytic sample, the overall weighted prevalence of HIV was 32.4% (n = 941) and HSV-2 was 53.2% (n = 1529). TMLE estimates suggest that MMC was associated with 31% lower HIV prevalence (PR: 0.690; 95% CI: 0.614, 0.777) and 21.1% lower HSV-2 prevalence (PR: 0.789; 95% CI: 0.734, 0.848). The propensity score analyses also provided evidence of association of MMC with lower prevalence of HIV and HSV-2. For PSFM: HIV (PR: 0.689; 95% CI: 0.537, 0.885), and HSV-2 (PR: 0.832; 95% CI: 0.709, 0.975). For IPTW: HIV (PR: 0.708; 95% CI: 0.572, 0.875), and HSV-2 (PR: 0.837; 95% CI: 0.738, 0.949).
Conclusion: Using a TMLE approach, we present further evidence of a protective association of MMC against HIV and HSV-2 in this hyper-endemic South African setting. TMLE has the potential to enhance the evidence base for recommendations that embrace the effect of public health interventions on health or disease outcomes.
Keywords: Full matching; IPTW; Male circumcision; STI; South Africa; TMLE.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Does voluntary medical male circumcision protect against sexually transmitted infections among men and women in real-world scale-up settings? Findings of a household survey in KwaZulu-Natal, South Africa.BMJ Glob Health. 2019 May 30;4(3):e001389. doi: 10.1136/bmjgh-2019-001389. eCollection 2019. BMJ Glob Health. 2019. PMID: 31263584 Free PMC article.
-
Medical Male Circumcision and Associations Among Sexually Transmitted Infections Service Attendees.AIDS Behav. 2020 May;24(5):1422-1431. doi: 10.1007/s10461-019-02729-9. AIDS Behav. 2020. PMID: 31720907
-
A comparison of the prevalence of sexually transmitted infections among circumcised and uncircumcised adult males in Rustenburg, South Africa: a cross-sectional study.BMC Public Health. 2021 Apr 6;21(1):656. doi: 10.1186/s12889-021-10509-1. BMC Public Health. 2021. PMID: 33823828 Free PMC article.
-
The association between lack of male circumcision and risk for HIV infection: a review of the epidemiological data.Sex Transm Dis. 1994 Jul-Aug;21(4):201-10. doi: 10.1097/00007435-199407000-00004. Sex Transm Dis. 1994. PMID: 7974070 Review.
-
Male circumcision to reduce the risk of HIV and sexually transmitted infections among men who have sex with men.Curr Opin Infect Dis. 2010 Feb;23(1):45-52. doi: 10.1097/QCO.0b013e328334e54d. Curr Opin Infect Dis. 2010. PMID: 19935420 Review.
Cited by
-
Identifying Individuals at High Risk for HIV and Sexually Transmitted Infections With an Artificial Intelligence-Based Risk Assessment Tool.Open Forum Infect Dis. 2024 Jan 8;11(3):ofae011. doi: 10.1093/ofid/ofae011. eCollection 2024 Mar. Open Forum Infect Dis. 2024. PMID: 38440304 Free PMC article.
-
The Targeted Maximum Likelihood estimation to estimate the causal effects of the previous tuberculosis treatment in Multidrug-resistant tuberculosis in Sudan.PLoS One. 2023 Jan 17;18(1):e0279976. doi: 10.1371/journal.pone.0279976. eCollection 2023. PLoS One. 2023. PMID: 36649340 Free PMC article.
References
-
- Davis S, Toledo C, Lewis L, Maughan-Brown B, Ayalew K, Kharsany AB. Does voluntary medical male circumcision protect against sexually transmitted infections among men and women in real-world scale-up settings? Findings of a household survey in KwaZulu-Natal, South Africa. BMJ Glob Health. 2019;4(3):e001389. doi: 10.1136/bmjgh-2019-001389. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
