

Maximizing acceptance of clinical pharmacy recommendations to reduce length of hospital stay in a private hospital from Amman, Jordan
- PMID: 34496856
- PMCID: PMC8424814
- DOI: 10.1186/s12913-021-06966-4
Maximizing acceptance of clinical pharmacy recommendations to reduce length of hospital stay in a private hospital from Amman, Jordan
Abstract
Background: Clinical pharmacy interventions (CPI) usually require prior medical authorization. Physicians approve 80% of CPI and reject 20%. If pharmacists show that physicians should authorize all 100% CPI, the profession will step closer to a fully independent prescriber status. This study used an artificial neural network (ANN) model to determine whether clinical pharmacy (CP) may improve outcomes associated with rejected CPI.
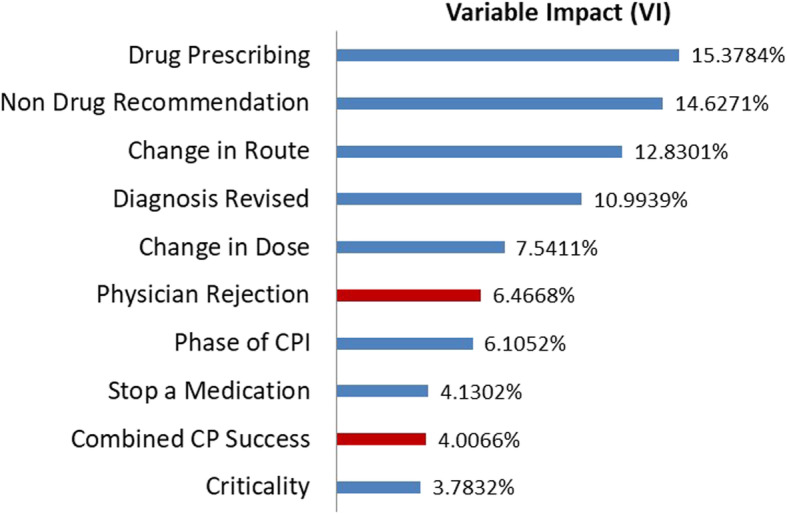
Method: This is a non-interventional, retrospective analysis of documented CPI in a 100-bed, acute-care private hospital in Amman, Jordan. Study consisted of 542 patients, 574 admissions, and 1694 CPI. Team collected demographic and clinical data using a standardized tool. Input consisted of 54 variables with some taking merely repetitive values for each CPI in each patient whereas others varying with every CPI. Therefore, CPI was consolidated to one rejected and/or one accepted per patient per admission. Groups of accepted and rejected CPI were compared in terms of matched and unmatched variables. ANN were, subsequently, trained and internally as well as cross validated for outcomes of interest. Outcomes were length of hospital and intensive care stay after the index CPI (LOSTA & LOSICUA, respectively), readmissions, mortality, and cost of hospitalization. Best models were finally used to compare the two scenarios of approving 80% versus 100% of CPI. Variable impacts (VI) automatically generated by the ANN were compared to evaluate the effect of rejecting CPI. Main outcome measure was Lengths of hospital stay after the index CPI (LOSTA).
Results: ANN configurations converged within 18 s and 300 trials. All models showed a significant reduction in LOSTA with 100% versus 80% accepted CPI of about 0.4 days (2.6 ± 3.4, median (range) of 2 (0-28) versus 3.0 ± 3.8, 2 (0-30), P-value = 0.022). Average savings with acceptance of those rejected CPI was 55 JD (~ 78 US dollars) and could help hire about 1.3 extra clinical pharmacist full-time equivalents.
Conclusions: Maximizing acceptance of CPI reduced the length of hospital stay in this model. Practicing Clinical Pharmacists may qualify for further privileges including promotion to a fully independent prescriber status.
Keywords: Acceptance; Clinical pharmacy interventions; Hospitalization; Jordan; Length of stay; Neural networks; Patient readmission; Pharmacists; Private hospital.
© 2021. The Author(s).
Conflict of interest statement
All authors have no competing interests to disclose.
Figures



References
-
- Bond CA, Raehl CL, Franke T. Interrelationships among mortality rates, drug costs, total cost of care, and length of stay in United States hospitals: summary and recommendations for clinical pharmacy services and staffing. Pharmacotherapy. 2001;21(2):129–141. doi: 10.1592/phco.21.2.129.34105. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
