

Subtotal cholecystectomy for difficult acute cholecystitis: how to finalize safely by laparoscopy-a systematic review
- PMID: 34496916
- PMCID: PMC8424983
- DOI: 10.1186/s13017-021-00392-x
Subtotal cholecystectomy for difficult acute cholecystitis: how to finalize safely by laparoscopy-a systematic review
Abstract
Background: Aim of this study was to clarify the best laparoscopic subtotal cholecystectomy (LSTC) technique for finalizing a difficult cholecystectomy.
Patients and methods: A review was performed (1987-2021) searching "difficulty cholecystectomy" AND/OR "subtotal cholecystectomy". The LSTC techniques considered were as follows: type A, leaving posterior wall attached to the liver and the remainder of the gallbladder stump open; type B, like type A but with the stump closed; type C, resection of both the anterior and posterior gallbladder walls and the stump closed; type D, like type C but with the stump open. Morbidity (including mortality) was analysed with Dindo-Clavien classification.
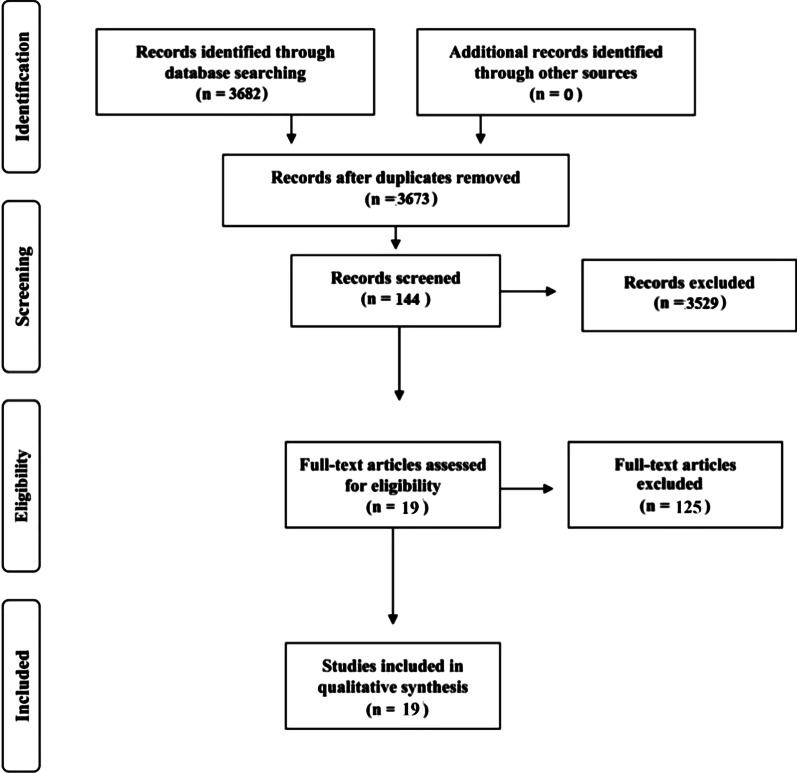
Results: Nineteen articles were included. Of the 13,340 patients screened, 678 (8.2%) had cholecystectomy finalized by LSTC: 346 patients (51.0%) had type A LSTC, 134 patients (19.8%) had type B LSTC, 198 patients (29.2%) had type C LSTC, and 198 patients (0%) had type D LSTC. Bile leakage was found in 83 patients (12.2%), and recorded in 58 patients (69.9%) treated by type A. Twenty-three patients (3.4%) developed a subhepatic collection, 19 of whom (82.6%) were treated by type A. Other complications were reported in 72 patients (10.6%). The Dindo-Clavien classification was four for grade I, 27 for grade II, 126 for grade IIIa, 18 for grade IIIb, zero for grade IV and three for grade V.
Conclusion: In the case of LSTC, closure of the gallbladder stump represents the best method to avoid complications. Careful exploration of the gallbladder stump is mandatory, washing the abdominal cavity and leaving drainage.
Keywords: Clavien–Dindo classification; Complications; Difficulty cholecystectomy; Gallbladder; Laparoscopic subtotal cholecystectomy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Successful procedure with additional omentopexy to suture closure of gallbladder stump in laparoscopic subtotal cholecystectomy.Asian J Endosc Surg. 2022 Apr;15(2):372-375. doi: 10.1111/ases.13007. Epub 2021 Nov 2. Asian J Endosc Surg. 2022. PMID: 34726321 Free PMC article.
-
Laparoscopic subtotal cholecystectomy after percutaneous transhepatic gallbladder drainage for grade II or III acute cholecystitis.BMC Surg. 2021 Oct 30;21(1):386. doi: 10.1186/s12893-021-01387-w. BMC Surg. 2021. PMID: 34717615 Free PMC article.
-
A systematic review on laparoscopic subtotal cholecystectomy for difficult gallbladders: a lifesaving bailout or an incomplete operation?Ann R Coll Surg Engl. 2024 Mar;106(3):205-212. doi: 10.1308/rcsann.2023.0008. Epub 2023 Jun 27. Ann R Coll Surg Engl. 2024. PMID: 37365939 Free PMC article.
-
Laparoscopic Subtotal Cholecystectomy for the Difficult Gallbladder: A Safe Alternative.Isr Med Assoc J. 2020 Sep;22(9):538-541. Isr Med Assoc J. 2020. PMID: 33236550
-
2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis.World J Emerg Surg. 2020 Nov 5;15(1):61. doi: 10.1186/s13017-020-00336-x. World J Emerg Surg. 2020. PMID: 33153472 Free PMC article. Review.
Cited by
-
Laparoscopic subtotal reconstituting cholecystectomy in type II & III Mirizzi syndrome: Case series of 5 patients.Int J Surg Case Rep. 2022 Aug;97:107425. doi: 10.1016/j.ijscr.2022.107425. Epub 2022 Jul 21. Int J Surg Case Rep. 2022. PMID: 35872547 Free PMC article.
-
Laparoscopic Management of Cholecystoduodenal and Cholecystocolic Fistula: A Clinical Case Report.Cureus. 2023 Jun 19;15(6):e40657. doi: 10.7759/cureus.40657. eCollection 2023 Jun. Cureus. 2023. PMID: 37476135 Free PMC article.
-
State of the art in subtotal cholecystectomy: An overview.Front Surg. 2023 Apr 21;10:1142579. doi: 10.3389/fsurg.2023.1142579. eCollection 2023. Front Surg. 2023. PMID: 37151864 Free PMC article. Review.
-
Development and validation of a radiologically-based nomogram for preoperative prediction of difficult laparoscopic cholecystectomy.Front Med (Lausanne). 2025 Apr 22;12:1561769. doi: 10.3389/fmed.2025.1561769. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40342585 Free PMC article.
-
Cesena guidelines: WSES consensus statement on laparoscopic-first approach to general surgery emergencies and abdominal trauma.World J Emerg Surg. 2023 Dec 8;18(1):57. doi: 10.1186/s13017-023-00520-9. World J Emerg Surg. 2023. PMID: 38066631 Free PMC article.
References
-
- Purzner RH, Ho KB, Al-Sukhni E, Jayaraman S. Safe laparoscopic subtotal cholecystectomy in the face of severe inflammation in the cystohepatic triangle: a retrospective review and proposed management strategy for the difficult gallbladder. Can J Surg. 2019;62:402–411. doi: 10.1503/cjs.014617. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
