

External validation of the 4C Mortality Score for patients with COVID-19 and pre-existing cardiovascular diseases/risk factors
- PMID: 34497086
- PMCID: PMC8438580
- DOI: 10.1136/bmjopen-2021-052708
External validation of the 4C Mortality Score for patients with COVID-19 and pre-existing cardiovascular diseases/risk factors
Abstract
Objectives: Predictive algorithms to inform risk management decisions are needed for patients with COVID-19, although the traditional risk scores have not been adequately assessed in Asian patients. We aimed to evaluate the performance of a COVID-19-specific prediction model, the 4C (Coronavirus Clinical Characterisation Consortium) Mortality Score, along with other conventional critical care risk models in Japanese nationwide registry data.
Design: Retrospective cohort study.
Setting and participants: Hospitalised patients with COVID-19 and cardiovascular disease or coronary risk factors from January to May 2020 in 49 hospitals in Japan.
Main outcome measures: Two different types of outcomes, in-hospital mortality and a composite outcome, defined as the need for invasive mechanical ventilation and mortality.
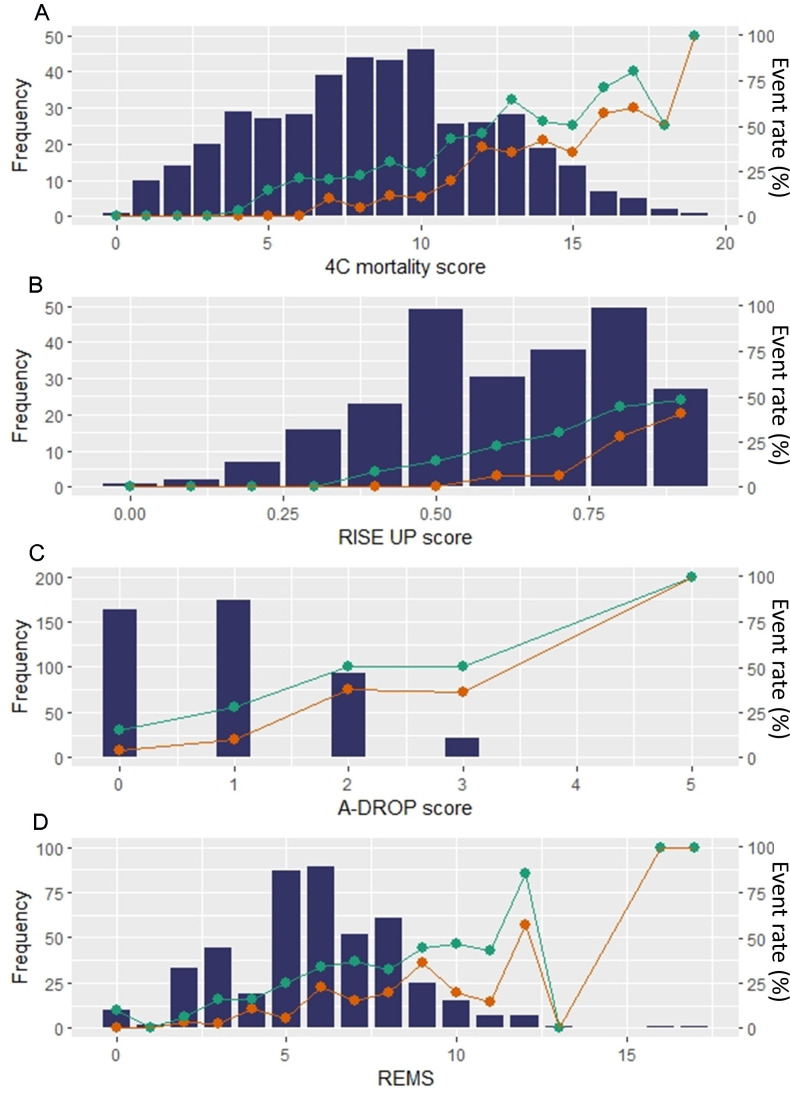
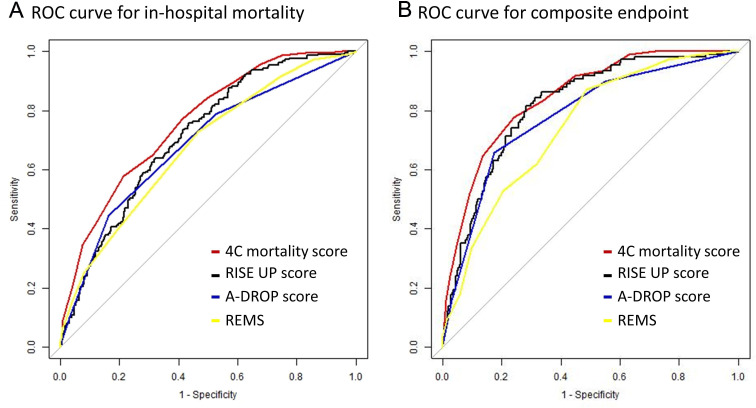
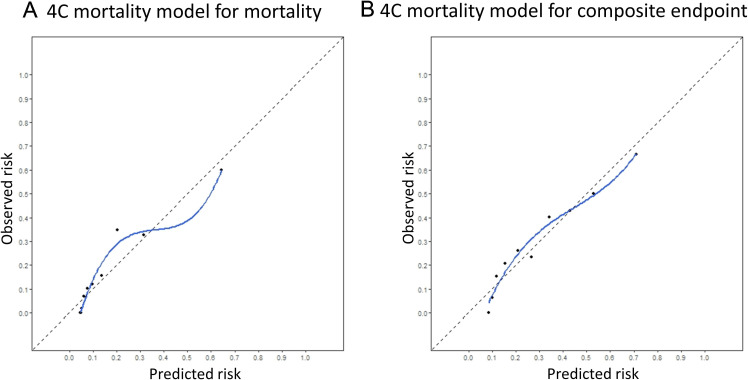
Results: The risk scores for 693 patients were tested by predicting in-hospital mortality for all patients and composite endpoint among those not intubated at baseline (n=659). The number of events was 108 (15.6%) for mortality and 178 (27.0%) for composite endpoints. After missing values were multiply imputed, the performance of the 4C Mortality Score was assessed and compared with three prediction models that have shown good discriminatory ability (RISE UP score, A-DROP score and the Rapid Emergency Medicine Score (REMS)). The area under the receiver operating characteristic curve (AUC) for the 4C Mortality Score was 0.84 (95% CI 0.80 to 0.88) for in-hospital mortality and 0.78 (95% CI 0.74 to 0.81) for the composite endpoint. It showed greater discriminatory ability compared with other scores, except for the RISE UP score, for predicting in-hospital mortality (AUC: 0.82, 95% CI 0.78 to 0.86). Similarly, the 4C Mortality Score showed a positive net reclassification improvement index over the A-DROP and REMS for mortality and over all three scores for the composite endpoint. The 4C Mortality Score model showed good calibration, regardless of outcome.
Conclusions: The 4C Mortality Score performed well in an independent external COVID-19 cohort and may enable appropriate disposition of patients and allocation of medical resources.Trial registration number UMIN000040598.
Keywords: COVID-19; epidemiology; respiratory infections.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: TY belongs to endowed departments of Abbott Vascular Japan, Boston Scientific Japan, Japan Lifeline, WIN International and Takeyama KK. SKo received unrestricted research grants from the Department of Cardiology, Keio University School of Medicine provided by Daiichi Sankyo and Bristol Myers Squibb, and lecture fees from AstraZeneca and Bristol Myers Squibb. ST received unrestricted research grants from Japan Medical Device Technology, Boston Scientific Japan and Asahi Intecc, and received an honorarium from Boston Scientific Japan, Abbott Vascular Japan and Medtronic. IK received unrestricted research grants from Daiichi Sankyo, Sumitomo Dainippon Pharma, Takeda Pharmaceutical Company, Mitsubishi Tanabe Pharma Corporation, Teijin Pharma, Idorsia Pharmaceuticals, Otsuka Pharmaceutical, Bayer Yakuhin, Ono Pharmaceutical and Toa Eiyo, and lecture fees from AstraZeneca, Daiichi Sankyo Company, Takeda Pharmaceutical Company, Bayer Yakuhin, Pfizer Japan and Ono Pharmaceutical. KN received lecture fees from Astellas, AstraZeneca, Bayer Yakuhin, Boehringer Ingelheim Japan, Daiichi Sankyo, Eli Lilly Japan Kowa, Mitsubishi Tanabe Pharma, MSD, Novartis Pharma, Ono Pharmaceutical, Otsuka and Takeda Pharmaceutical, research funding from Asahi Kasei, Astellas, Boehringer Ingelheim Japan, Mitsubishi Tanabe Pharma, Teijin Pharma and Terumo Corporation, and scholarship funds from Bayer Yakuhin, Daiichi Sankyo, Medtronic, Takeda Pharmaceutical and Teijin Pharma. YM is affiliated with a department endowed by Philips Respironics, ResMed, Teijin Home Healthcare and Fukuda Denshi, received an honorarium from Otsuka Pharmaceutical and Novartis Japan, received consultant fee from Otsuka Pharmaceutical, and joint research funds from Otsuka Pharmaceutical and Pfizer. IK, KH and KN are members of Circulation journal’s editorial team.
Figures
References
-
- WHO coronavirus (COVID-19) dashboard. Available: https://covid19.who.int
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical