Lung Function, Radiological Findings and Biomarkers of Fibrogenesis in a Cohort of COVID-19 Patients Six Months After Hospital Discharge
- PMID: 34497426
- PMCID: PMC8414844
- DOI: 10.1016/j.arbres.2021.08.014
Lung Function, Radiological Findings and Biomarkers of Fibrogenesis in a Cohort of COVID-19 Patients Six Months After Hospital Discharge
Abstract
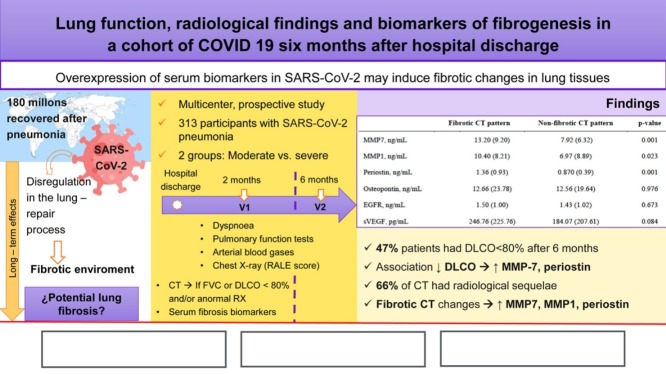
Introduction: Impairment in pulmonary function tests and radiological abnormalities are a major concern in COVID-19 survivors. Our aim is to evaluate functional respiratory parameters, changes in chest CT, and correlation with peripheral blood biomarkers involved in lung fibrosis at two and six months after SARS-CoV-2 pneumonia.
Methods: COVID-FIBROTIC (clinicaltrials.gov NCT04409275) is a multicenter prospective observational cohort study aimed to evaluate discharged patients. Pulmonary function tests, circulating serum biomarkers, chest radiography and chest CT were performed at outpatient visits.
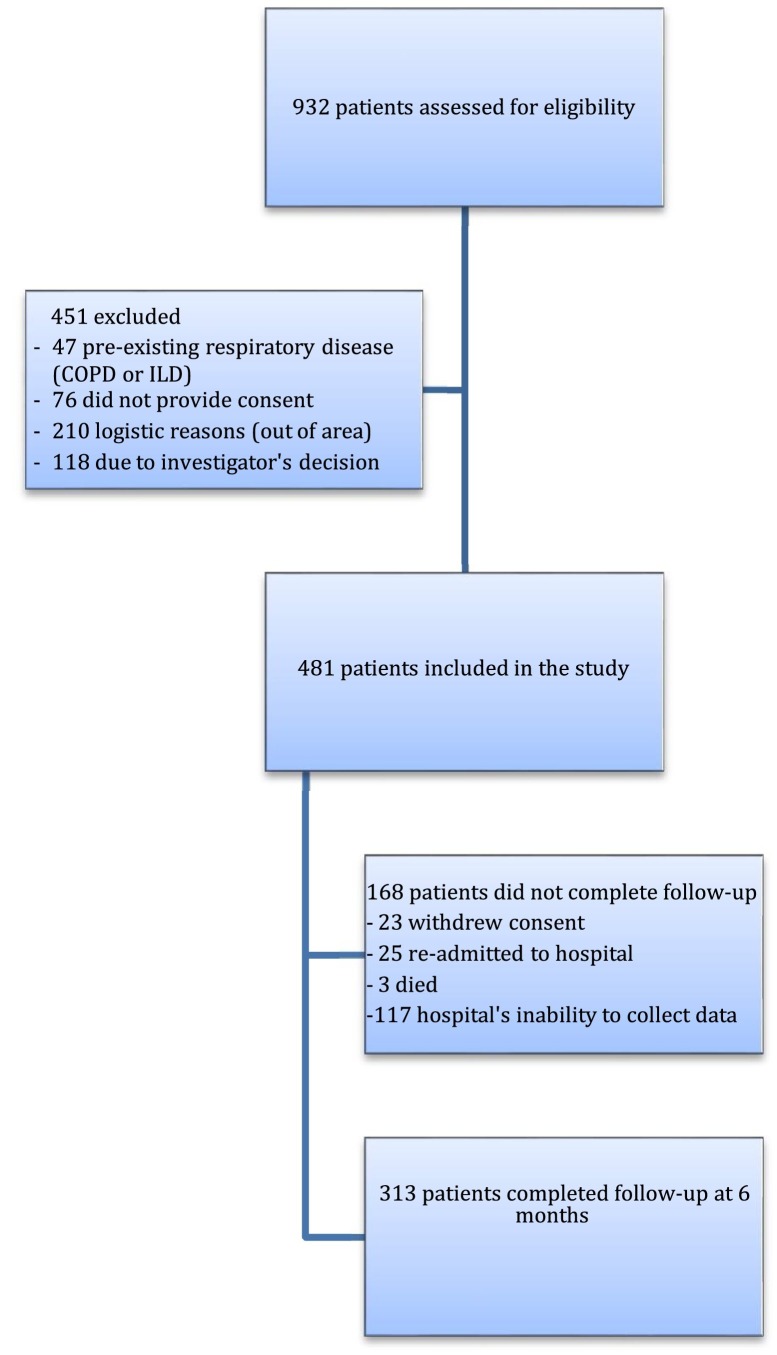
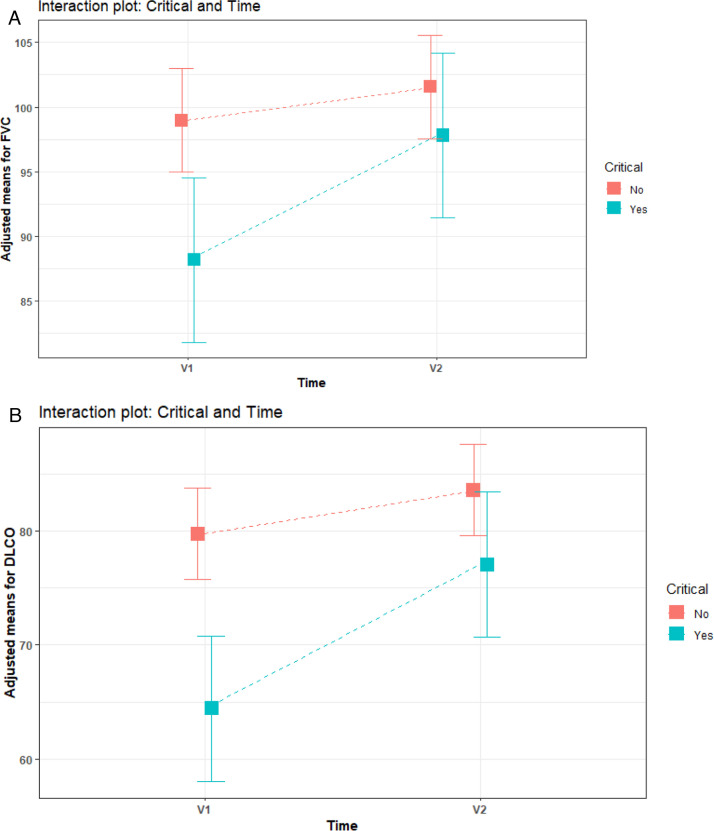
Results: In total, 313, aged 61.12 ± 12.26 years, out of 481 included patients were available. The proportion of patients with DLCO < 80% was 54.6% and 47% at 60 and 180 days. Associated factors with diffusion impairment at 6 months were female sex (OR: 2.97, 95%CI 1.74-5.06, p = 0.001), age (OR: 1.03, 95% CI: 1.01-1.05, p = 0.005), and peak RALE score (OR: 1.22, 95% CI 1.06-1.40, p = 0.005). Patients with altered lung diffusion showed higher levels of MMP-7 (11.54 ± 8.96 vs 6.71 ± 4.25, p = 0.001), and periostin (1.11 ± 0.07 vs 0.84 ± 0.40, p = 0.001). 226 patients underwent CT scan, of whom 149 (66%) had radiological sequelae of COVID-19. In severe patients, 68.35% had ground glass opacities and 38.46% had parenchymal bands. Early fibrotic changes were associated with higher levels of MMP7 (13.20 ± 9.20 vs 7.92 ± 6.32, p = 0.001), MMP1 (10.40 ± 8.21 vs 6.97 ± 8.89, p = 0.023), and periostin (1.36 ± 0.93 vs 0.87 ± 0.39, p = 0.001).
Conclusion: Almost half of patients with moderate or severe COVID-19 pneumonia had impaired pulmonary diffusion six months after discharge. Severe patients showed fibrotic lesions in CT scan and elevated serum biomarkers involved in pulmonary fibrosis.
Introducción: El deterioro de la función pulmonar en las pruebas correspondientes y las alteraciones radiológicas son las preocupaciones principales en los supervivientes de la COVID-19. Nuestro objetivo fue evaluar los parámetros de la función respiratoria, los cambios en la TC de tórax y la correlación con los biomarcadores en sangre periférica involucrados en la fibrosis pulmonar a los 2 y a los 6 meses tras la neumonía por SARS-CoV-2.
Métodos: El ensayo COVID-FIBROTIC (clinicaltrials.gov NCT04409275) es un estudio de cohortes multicéntrico, prospectivo y observacional cuyo objetivo fue evaluar los pacientes dados de alta. Se realizaron pruebas de función pulmonar, detección de biomarcadores en plasma circulante y radiografía y TC de tórax durante las visitas ambulatorias.
Resultados: En total 313 pacientes, de 61,12 ± 12,26 años, de los 481 incluidos estuvieron disponibles.La proporción de pacientes con DLCO < 80% fue del 54,6 y del 47% a los 60 y 180 días.Los factores que se asociaron a la alteración de la difusión a los 6 meses fueron el sexo femenino (OR: 2,97; IC del 95%: 1,74-5,06; p = 0,001), la edad (OR: 1,03; IC del 95%: 1,01-1,05; p = 0,005) y la puntuación RALE más alta (OR: 1,22; IC del 95%: 1,06-1,40; p = 0,005). Los pacientes con alteración de la difusión pulmonar mostraron niveles más altos de MMP-7 (11,54 ± 8,96 frente a 6,71 ± 4,25; p = 0,001) y periostina (1,11 ± 0.07 frente a 0,84 ± 0,40; p = 0,001). Se le realizó una TC a 226 pacientes de los cuales 149 (66%) presentaban secuelas radiológicas de la COVID-19. En los pacientes graves, el 68,35% mostraban opacidades en vidrio esmerilado y el 38,46%, bandas parenquimatosas. Los cambios fibróticos tempranos se asociaron a niveles más altos de MMP7 (13,20 ± 9,20 frente a 7,92 ± 6,32; p = 0,001), MMP1 (10,40 ± 8,21 frente a 6,97 ± 8,89; p = 0,023), y periostina (1,36 ± 0,93 frente a 0,87 ± 0,39; p = 0,001).
Conclusión: Casi la mitad de los pacientes con neumonía moderada o grave por COVID-19 presentaba alteración de la difusión pulmonar 6 meses después del alta. Los pacientes graves mostraban lesiones fibróticas en laTC y un aumento de los biomarcadores séricos relacionados con la fibrosis pulmonar.
Keywords: 6-MWT, 6 minute-walk test; ARDS, acute respiratory distress syndrome; BMI, body mass index; COPD, chronic obstructive pulmonary disease; COVID-19 sequelae; COVID-19, coronavirus disease 2019; CT, computed tomography; Chest CT; DLCO, diffusing capacity for carbon monoxide; Fibrotic changes; GGO, ground-glass opacity; HFNC, high flow nasal cannula oxygen; ILD, interstitial lung disease; IMV, mechanical ventilation; Interstitial lung disease; Lung diffusion; MMP, matrix metalloproteinases; NIV, non-invasive ventilation; RALE, radiographic assessment of lung edema; RT-PCR, reverse transcriptase-polymerase chain reaction; SARS, severe acute respiratory syndrome; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; Serum biomarkers; VEGF, vascular endothelial growth factor; mMRC, modified British Medical Research Council; sEGFR, soluble epidermal growth factor receptor.
© 2021 SEPAR. Published by Elsevier España, S.L.U. All rights reserved.
Figures
References
-
- https://coronavirus.jhu.edu/map.html [accessed 11.8.21].
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous