

Effects of Prior Antiplatelet Therapy on Mortality, Functional Outcome, and Hematoma Expansion in Intracerebral Hemorrhage: An Updated Systematic Review and Meta-Analysis of Cohort Studies
- PMID: 34497575
- PMCID: PMC8419415
- DOI: 10.3389/fneur.2021.691357
Effects of Prior Antiplatelet Therapy on Mortality, Functional Outcome, and Hematoma Expansion in Intracerebral Hemorrhage: An Updated Systematic Review and Meta-Analysis of Cohort Studies
Abstract
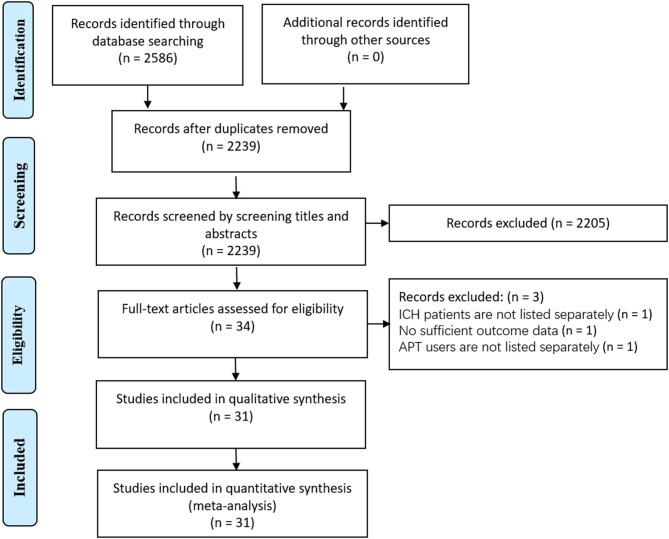
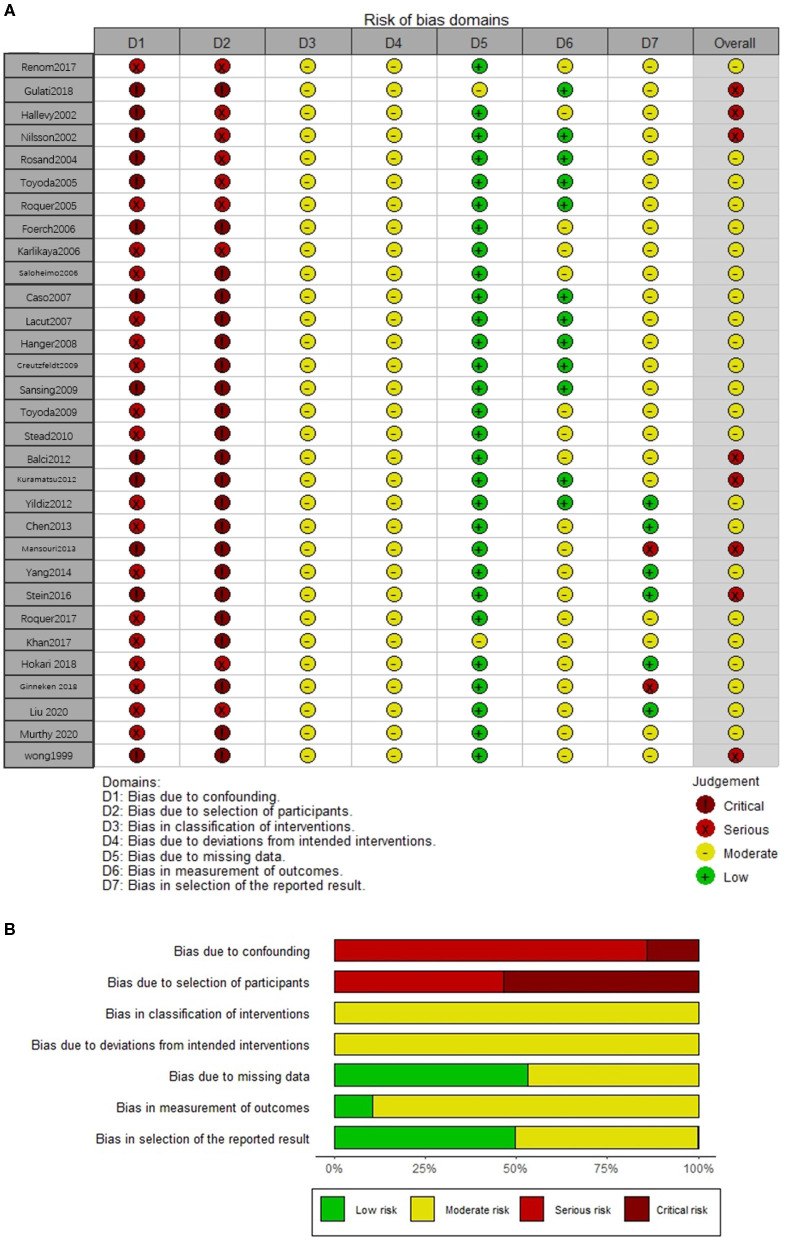
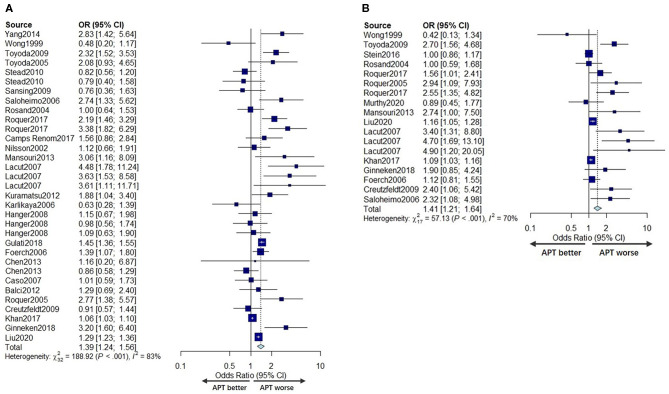
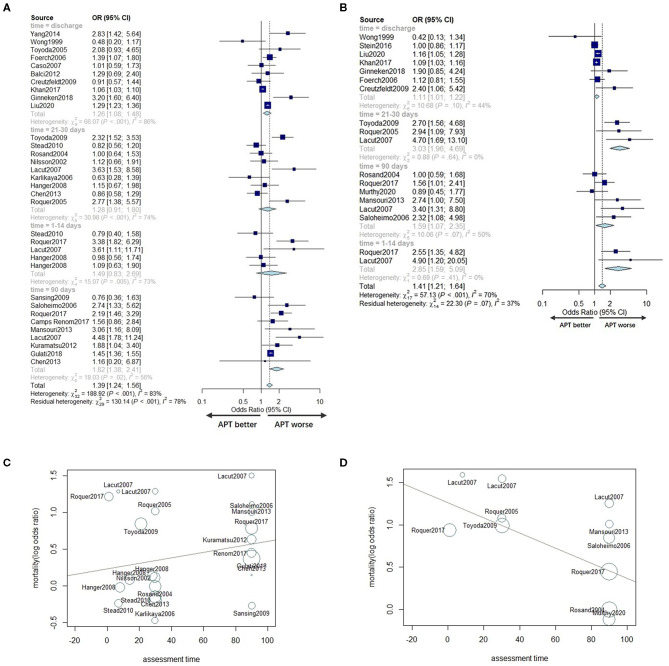
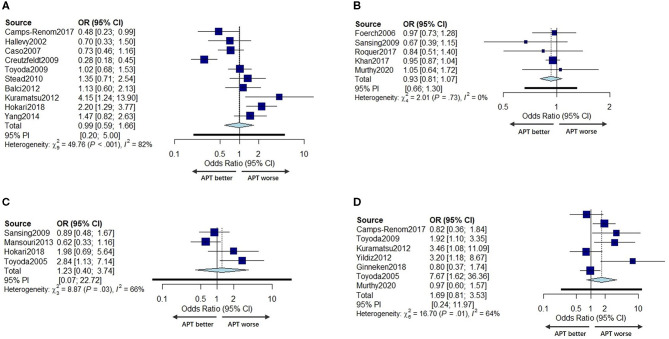
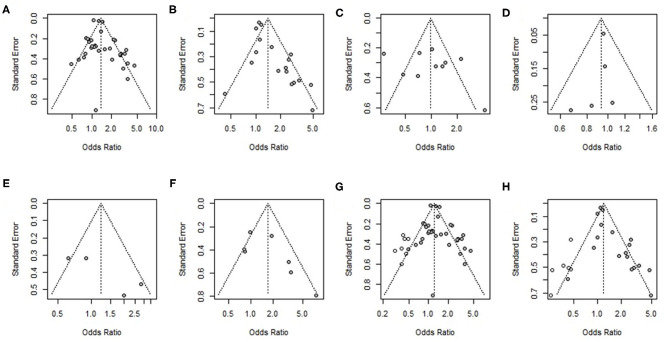
Background and Objective: Antiplatelet therapy (APT) is widely used and believed to be associated with increased poor prognosis by promoting bleeding in patients with intracerebral hemorrhage (ICH). We performed a systematic review and meta-analysis to determine whether prior APT is associated with mortality, functional outcome, and hematoma expansion in ICH patients. Methods: The PubMed, Embase, and Web of Science databases were searched for relevant published studies up to December 11, 2020. Univariate and multivariable adjusted odds ratios (ORs) were pooled using a random effects model. Cochran's chi-squared test (Cochran's Q), the I 2 statistic, and meta-regression analysis were used to evaluate the heterogeneity. Meta-regression models were developed to explore sources of heterogeneity. Funnel plots were used to detect publication bias. A trim-and-fill method was performed to identify possible asymmetry and assess the robustness of the conclusions. Results: Thirty-one studies fulfilled the inclusion criteria and exhibited a moderate risk of bias. Prior APT users with intracerebral hemorrhage (ICH) had a slightly increased mortality in both univariate analyses [odds ratio (OR) 1.39, 95% CI 1.24-1.56] and multivariable adjusted analyses (OR 1.41, 95% CI 1.21-1.64). The meta-regression indicated that for each additional day of assessment time, the adjusted OR for the mortality of APT patients decreased by 0.0089 (95% CI: -0.0164 to -0.0015; P = 0.0192) compared to that of non-APT patients. However, prior APT had no effects on poor function outcome (pooled univariate OR: 0.99, 95% CI 0.59-1.66; pooled multivariable adjusted OR: 0.93, 95% CI 0.87-1.07) or hematoma growth (pooled univariate OR: 1.23, 95% CI 0.40-3.74, pooled multivariable adjusted OR: 0.94, 95% CI 0.24-3.60). Conclusions: Prior APT was not associated with hematoma expansion or functional outcomes, but there was modestly increased mortality in prior APT patients. Higher mortality of prior APT patients was related to the strong influence of prior APT use on early mortality. Systematic Review Registration:PROSPERO Identifier [CRD42020215243].
Keywords: antiplatelet therapy; functional outcome; hematoma expansion; intracerebral hemorrhage; mortality.
Copyright © 2021 Wu, Zhang, Chen, Liu and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of Prior Antiplatelet Therapy on the Prognosis of Primary Intracerebral Hemorrhage: A Meta-analysis.Chin Med J (Engl). 2017 Dec 20;130(24):2969-2977. doi: 10.4103/0366-6999.220302. Chin Med J (Engl). 2017. PMID: 29237930 Free PMC article.
-
Does prior antiplatelet therapy influence hematoma volume and hematoma growth following intracerebral hemorrhage? Results from a prospective study and a meta-analysis.Eur J Neurol. 2017 Feb;24(2):302-308. doi: 10.1111/ene.13193. Epub 2016 Nov 1. Eur J Neurol. 2017. PMID: 27801531
-
Prior antiplatelet therapy is not associated with larger hematoma volume or hematoma growth in intracerebral hemorrhage.Neurol Sci. 2018 Apr;39(4):745-748. doi: 10.1007/s10072-018-3255-z. Epub 2018 Feb 14. Neurol Sci. 2018. PMID: 29441487
-
Island Sign Predicts Hematoma Expansion and Poor Outcome After Intracerebral Hemorrhage: A Systematic Review and Meta-Analysis.Front Neurol. 2020 Jun 4;11:429. doi: 10.3389/fneur.2020.00429. eCollection 2020. Front Neurol. 2020. PMID: 32582001 Free PMC article.
-
Effect of antiplatelet therapy on the incidence, prognosis, and rebleeding of intracerebral hemorrhage.CNS Neurosci Ther. 2023 Jun;29(6):1484-1496. doi: 10.1111/cns.14175. Epub 2023 Mar 21. CNS Neurosci Ther. 2023. PMID: 36942509 Free PMC article. Review.
Cited by
-
Machine learning model prediction of 6-month functional outcome in elderly patients with intracerebral hemorrhage.Neurosurg Rev. 2022 Aug;45(4):2857-2867. doi: 10.1007/s10143-022-01802-7. Epub 2022 May 6. Neurosurg Rev. 2022. PMID: 35522333 Free PMC article.
-
Incidence and prognosis of first-ever intracerebral hemorrhage on antiplatelet therapy over 10 years in a population-based stroke registry.Sci Rep. 2024 Nov 29;14(1):29664. doi: 10.1038/s41598-024-81526-4. Sci Rep. 2024. PMID: 39614089 Free PMC article.
References
-
- Ducrocq G, Amarenco P, Labreuche J, Alberts MJ, Mas JL, Ohman EM, et al. . A history of stroke/transient ischemic attack indicates high risks of cardiovascular event and hemorrhagic stroke in patients with coronary artery disease. Circulation. (2013) 127:730–8. 10.1161/CIRCULATIONAHA.112.141572 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources