

Pulsed Radiation Therapy to Improve Systemic Control of Metastatic Cancer
- PMID: 34497773
- PMCID: PMC8419338
- DOI: 10.3389/fonc.2021.737425
Pulsed Radiation Therapy to Improve Systemic Control of Metastatic Cancer
Abstract
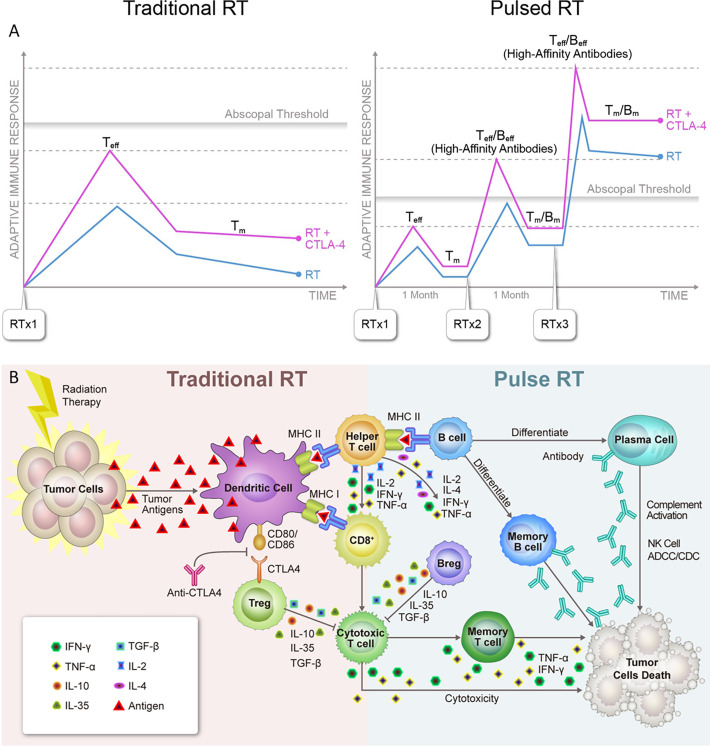
Radiation therapy (RT) is emerging as an interventional modality in the cancer-immunity cycle, augmenting the activation of an adaptive immune response against tumors. RT, particularly in combination with immunotherapy, can enhance immune memory effects and shape the tumor-directed T-cell populations. However, a single cycle of RT delivered to a limited number of polymetastatic lesions is rarely sufficient to achieve systemic control. We hypothesize that several rounds of RT, akin to several rounds of immunotherapeutic drugs, is likely to provide greater clinical benefit to patients with metastatic disease. We propose that the repeated exposure to tumor antigens released by "pulsed-RT" (i.e., treating 2-4 tumor lesions with 3 irradiation cycles given one month apart) may amplify the adaptive immune response by expanding the tumor-specific T-cell receptor repertoire, the production of high-affinity tumor antibodies, and the generation of memory lymphocytes and thereby improve immune control of systemic disease.
Keywords: adaptive immunity; immunotherapy; memory effect; metastatic cancer; radiation therapy.
Copyright © 2021 He, Barsoumian, Sezen, Puebla-Osorio, Hsu, Verma, Abana, Chen, Patel, Gu, Cortez and Welsh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Use of Multi-Site Radiation Therapy for Systemic Disease Control.Int J Radiat Oncol Biol Phys. 2021 Feb 1;109(2):352-364. doi: 10.1016/j.ijrobp.2020.08.025. Epub 2020 Aug 13. Int J Radiat Oncol Biol Phys. 2021. PMID: 32798606 Free PMC article. Review.
-
Integration of radiation and immunotherapy in breast cancer - Treatment implications.Breast. 2018 Apr;38:66-74. doi: 10.1016/j.breast.2017.12.005. Epub 2018 Jan 4. Breast. 2018. PMID: 29253718 Review.
-
Immune checkpoint inhibitors with radiotherapy and locoregional treatment: synergism and potential clinical implications.Curr Opin Oncol. 2015 Nov;27(6):445-51. doi: 10.1097/CCO.0000000000000225. Curr Opin Oncol. 2015. PMID: 26447875 Review.
-
Is Single-Site Radiation Therapy Enough to Augment the Immune System and Enhance Immunotherapy for Metastatic Disease?Semin Radiat Oncol. 2024 Jul;34(3):272-275. doi: 10.1016/j.semradonc.2024.05.003. Semin Radiat Oncol. 2024. PMID: 38880535 Review.
-
Addition of TLR9 agonist immunotherapy to radiation improves systemic antitumor activity.Transl Oncol. 2021 Feb;14(2):100983. doi: 10.1016/j.tranon.2020.100983. Epub 2020 Dec 16. Transl Oncol. 2021. PMID: 33340886 Free PMC article.
Cited by
-
Pulsed radiotherapy to mitigate high tumor burden and generate immune memory.Front Immunol. 2022 Oct 6;13:984318. doi: 10.3389/fimmu.2022.984318. eCollection 2022. Front Immunol. 2022. PMID: 36275767 Free PMC article.
-
Low-Dose Cyclophosphamide Enhances the Tumoricidal Effects of 5-Day Spacing Stereotactic Ablative Radiotherapy by Boosting Antitumor Immunity.Cancer Res Treat. 2025 Jul;57(3):678-692. doi: 10.4143/crt.2024.807. Epub 2024 Nov 8. Cancer Res Treat. 2025. PMID: 39512061 Free PMC article.
-
Efficacy and Safety of Immune Checkpoint Inhibitor Rechallenge in the Treatment of Esophageal Squamous Cell Cancer.J Cancer. 2025 Jan 1;16(3):943-951. doi: 10.7150/jca.104380. eCollection 2025. J Cancer. 2025. PMID: 39781362 Free PMC article.
-
Investigation of Normal Tissue Toxicity in Pulsed Low Dose Rate Radiotherapy.Cancers (Basel). 2025 May 19;17(10):1701. doi: 10.3390/cancers17101701. Cancers (Basel). 2025. PMID: 40427198 Free PMC article.
-
Particle Beam Radiobiology Status and Challenges: A PTCOG Radiobiology Subcommittee Report.Int J Part Ther. 2024 Aug 8;13:100626. doi: 10.1016/j.ijpt.2024.100626. eCollection 2024 Sep. Int J Part Ther. 2024. PMID: 39258166 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources