

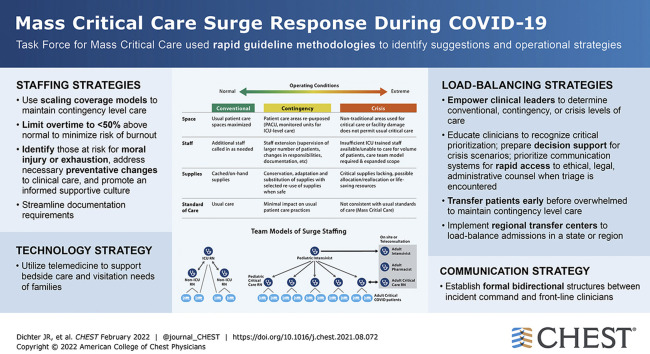
Mass Critical Care Surge Response During COVID-19: Implementation of Contingency Strategies - A Preliminary Report of Findings From the Task Force for Mass Critical Care
- PMID: 34499878
- PMCID: PMC8420082
- DOI: 10.1016/j.chest.2021.08.072
Mass Critical Care Surge Response During COVID-19: Implementation of Contingency Strategies - A Preliminary Report of Findings From the Task Force for Mass Critical Care
Abstract
Background: After the publication of a 2014 consensus statement regarding mass critical care during public health emergencies, much has been learned about surge responses and the care of overwhelming numbers of patients during the COVID-19 pandemic. Gaps in prior pandemic planning were identified and require modification in the midst of severe ongoing surges throughout the world.
Research question: A subcommittee from The Task Force for Mass Critical Care (TFMCC) investigated the most recent COVID-19 publications coupled with TFMCC members anecdotal experience in order to formulate operational strategies to optimize contingency level care, and prevent crisis care circumstances associated with increased mortality.
Study design and methods: TFMCC adopted a modified version of established rapid guideline methodologies from the World Health Organization and the Guidelines International Network-McMaster Guideline Development Checklist. With a consensus development process incorporating expert opinion to define important questions and extract evidence, the TFMCC developed relevant pandemic surge suggestions in a structured manner, incorporating peer-reviewed literature, "gray" evidence from lay media sources, and anecdotal experiential evidence.
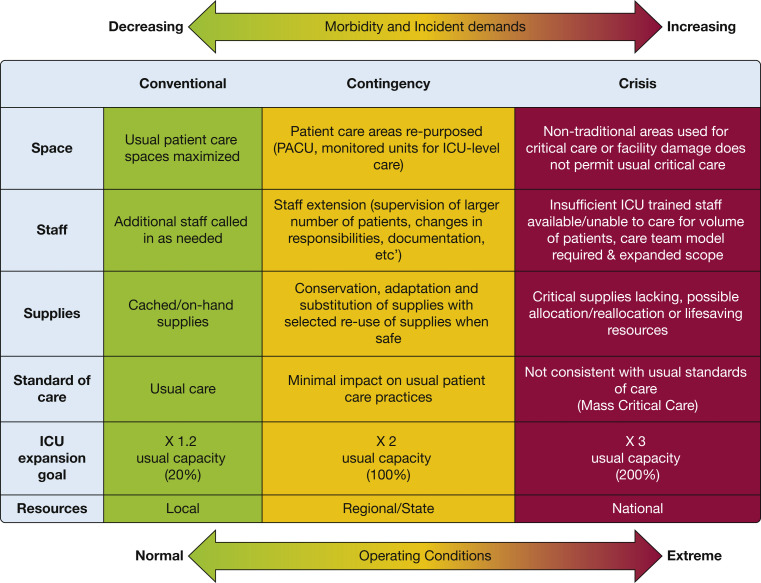
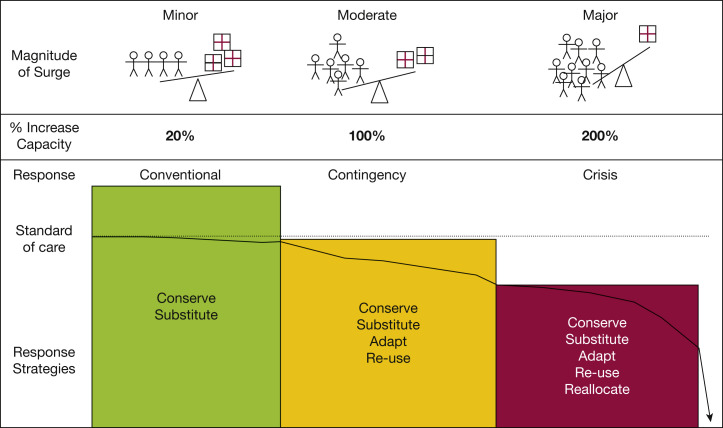
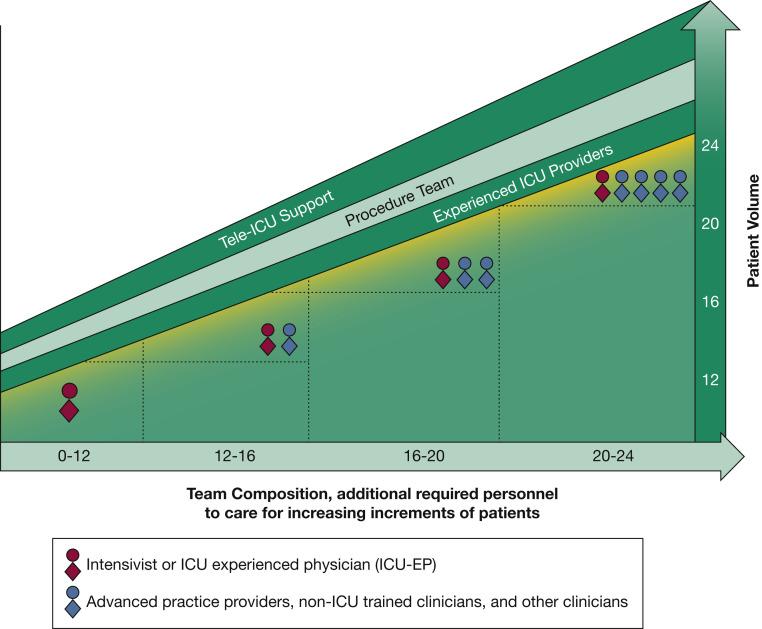
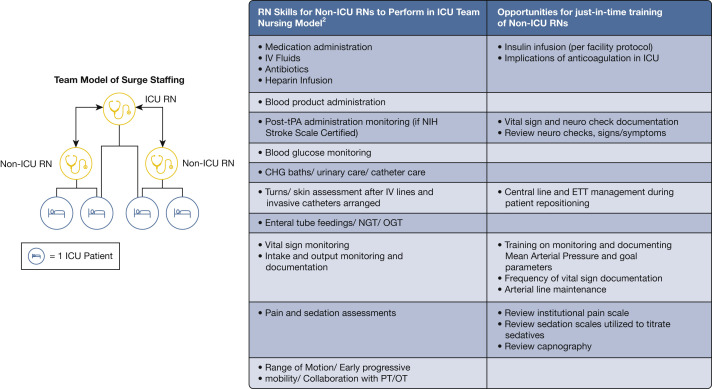
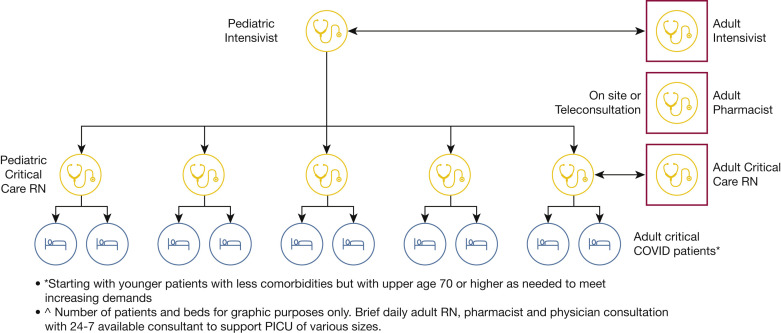
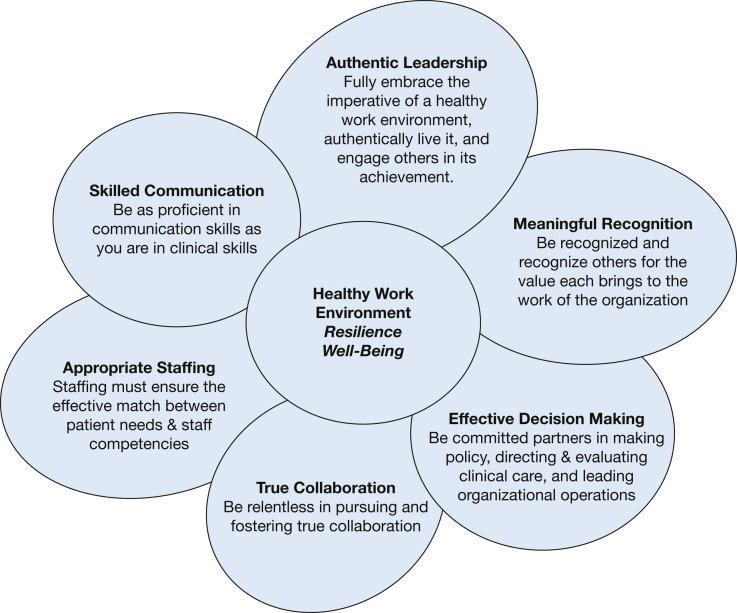
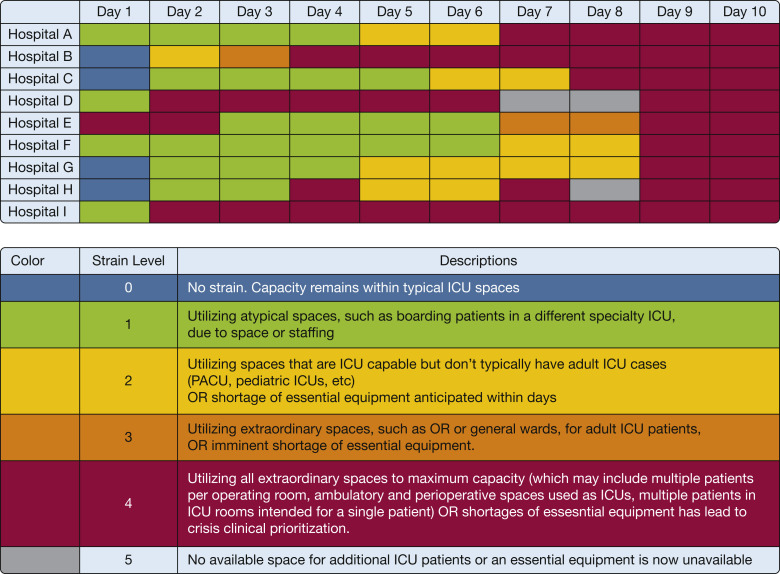
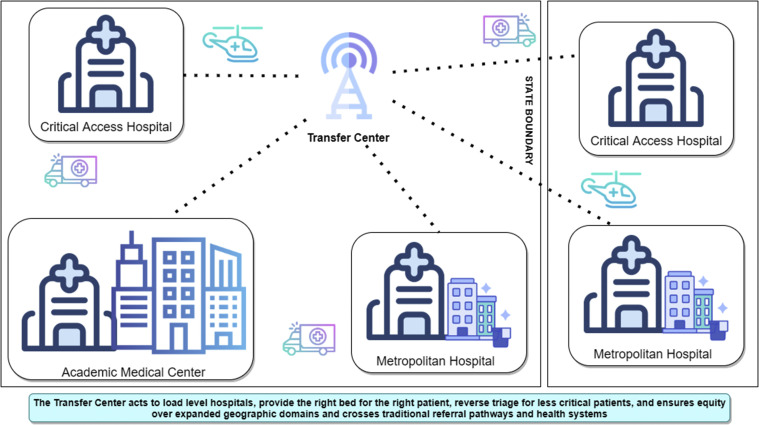
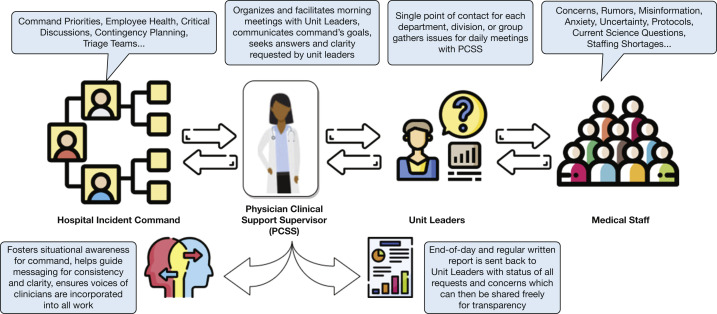
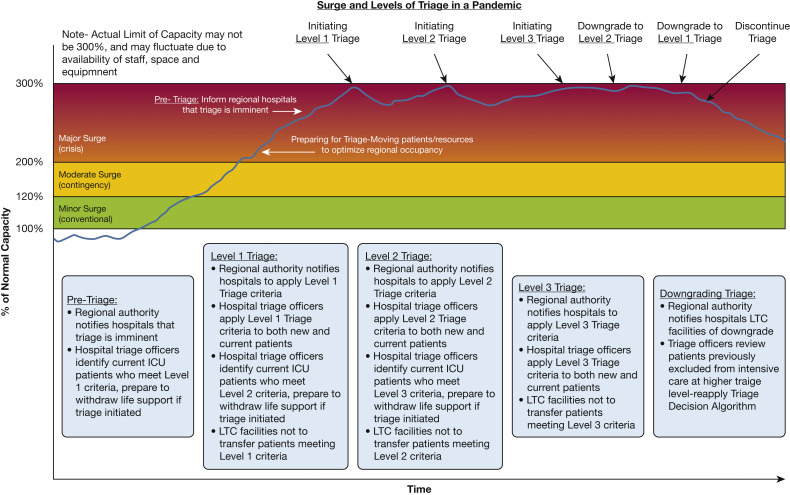
Results: Ten suggestions were identified regarding staffing, load-balancing, communication, and technology. Staffing models are suggested with resilience strategies to support critical care staff. ICU surge strategies and strain indicators are suggested to enhance ICU prioritization tactics to maintain contingency level care and to avoid crisis triage, with early transfer strategies to further load-balance care. We suggest that intensivists and hospitalists be engaged with the incident command structure to ensure two-way communication, situational awareness, and the use of technology to support critical care delivery and families of patients in ICUs.
Interpretation: A subcommittee from the TFMCC offers interim evidence-informed operational strategies to assist hospitals and communities to plan for and respond to surge capacity demands resulting from COVID-19.
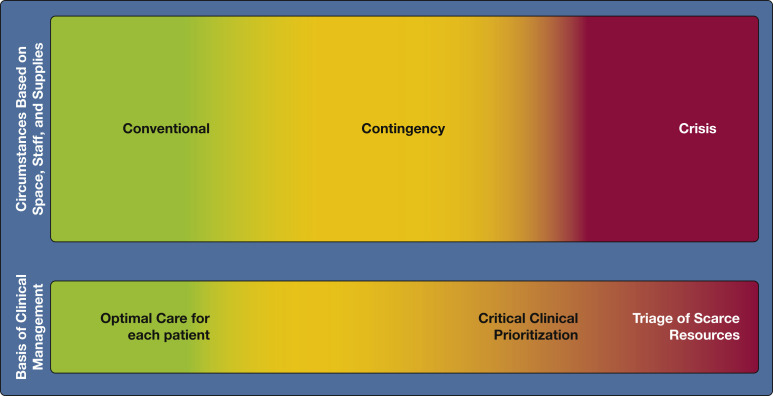
Keywords: COVID-19; contingency; conventional; crisis levels; critical clinical prioritization; incident command system; load-balancing; mass critical care; staffing; surge; telemedicine; tiered staffing.
Copyright © 2021 American College of Chest Physicians. All rights reserved.
Figures


References
-
- Hick J.L., Einav S., Hanfling D., et al. Surge capacity principles: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014;146(4 suppl):e1S–e16S. - PubMed
-
- Einav S., Hick J.L., Hanfling D., et al. Surge capacity logistics: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014;146(4 suppl):e17S–e43S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
