

The Comparison of Clinical Result between Primary Repair of the Anterior Cruciate Ligament with Additional Internal Bracing and Anatomic Single Bundle Reconstruction-A Retrospective Study
- PMID: 34501400
- PMCID: PMC8432121
- DOI: 10.3390/jcm10173948
The Comparison of Clinical Result between Primary Repair of the Anterior Cruciate Ligament with Additional Internal Bracing and Anatomic Single Bundle Reconstruction-A Retrospective Study
Abstract
Background: The current standard of treatment of anterior cruciate ligament (ACL) is reconstruction (ACLR). This technique has some disadvantages: poor proprioception, donor site morbidity and the inability to restore joint kinematics. ACL repair could be an alternative treatment. The purpose of the study was to compare the stability and the function after ACL primary repair versus single-bundle ACLR.
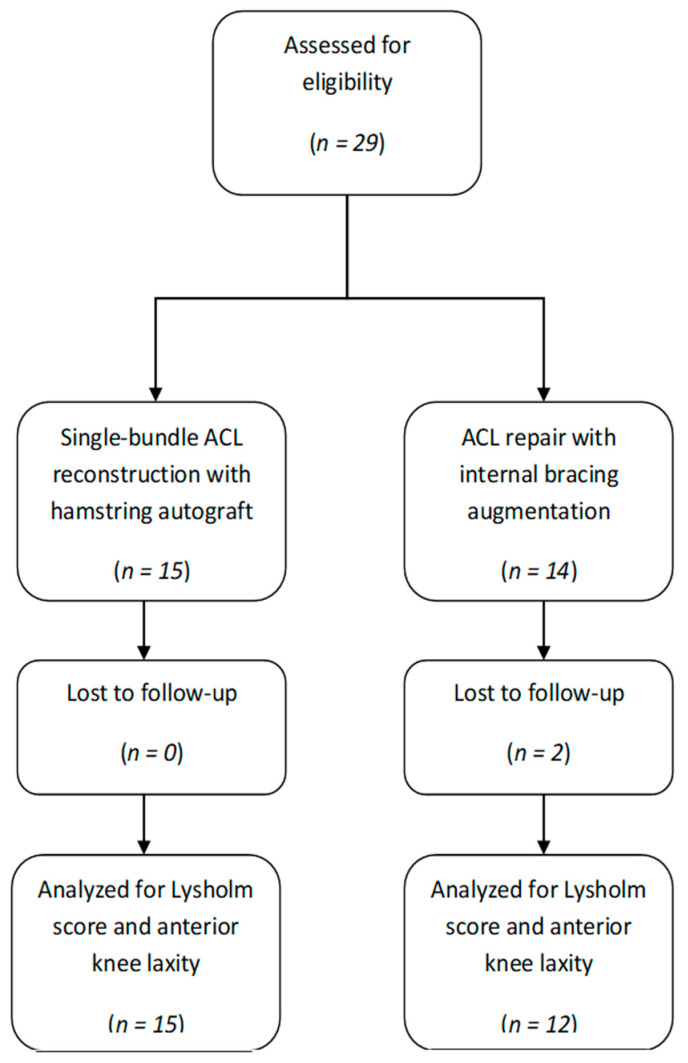
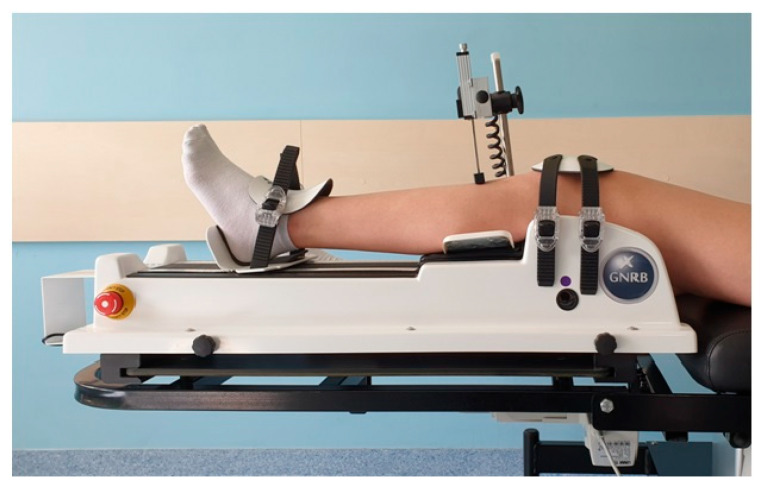
Methods: In a retrospective study, 12 patients underwent primary ACL repair with internal bracing, 15 patients underwent standard ACLR. Follow-up examinations were evaluated at up to 2 years postoperatively. One patient in the ACL repair group was lost to follow-up due to re-rupture. The absolute value of anterior tibial translation (ATT) and the side-to-side difference in the same patient (ΔATT) were evaluated using the GNRB arthrometer. The Lysholm knee scoring was obtained. Re-ruptures and other complications were recorded.
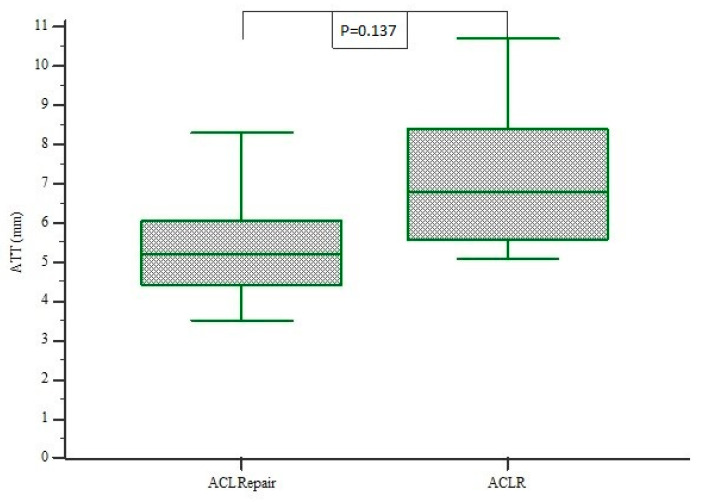
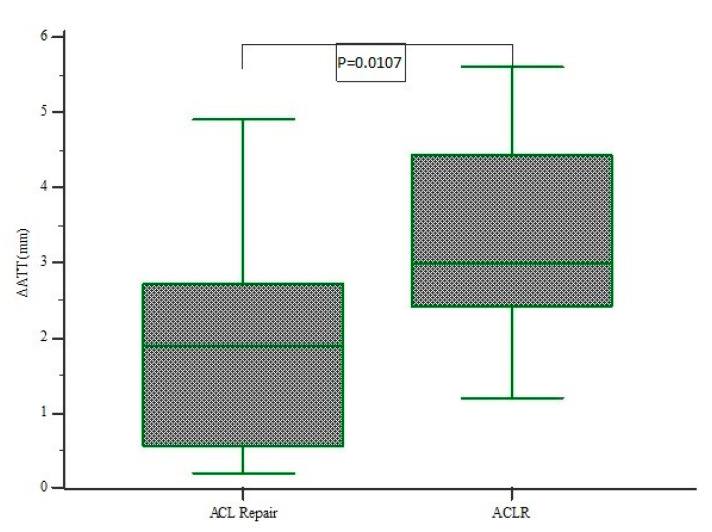
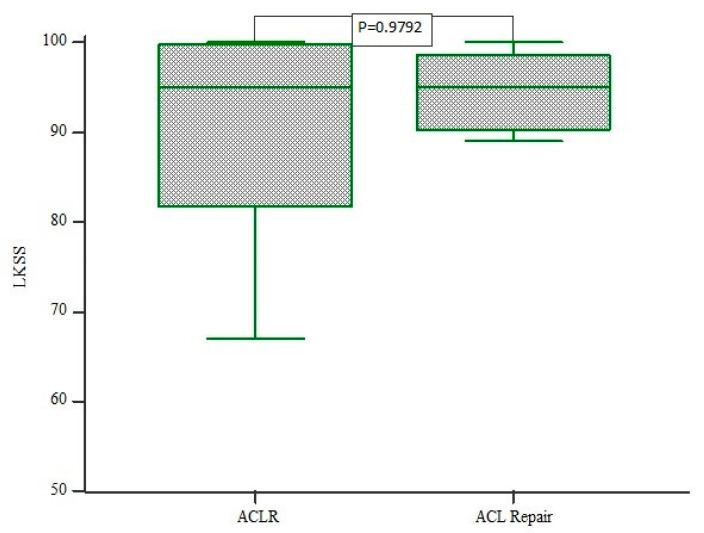
Results: Anterior tibial translation (ATT) was significantly decreased in the ACL repair group compared with the ACLR group (5.31 mm vs. 7.18 mm, respectively; p = 0.0137). Arthrometric measurements demonstrated a mean side-to-side difference (ΔATT) 1.87 (range 0.2 to 4.9) mm significantly decreased compared to ACLR 3.36 (range 1.2-5.6 mm; p = 0.0107). The mean Lysholm score was 85.3 points in the ACL repair group and 89.9 in ACLR group. No significant differences between ACL repair and ACLR were found for the Lysholm score. There was no association between AP laxity and clinical outcomes. There were two complications in the internal bracing group: one patient had re-rupture and was treated by ACLR, another had limited extension and had arthroscopic debridement.
Conclusions: Anterior tibial translation was significantly decreased after ACL repair. Additionally, the functional results after ACL repair with internal bracing were comparable with those after ACLR. It should be noted that the two complications occurred. The current study supports further development of ACL repair techniques.
Keywords: anterior cruciate ligament (ACL); internal bracing; knee laxity; primary ACL repair.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Murray M.M., Kalish L.A., Fleming B.C., Flutie B., Freiberger C., Henderson R.N., Perrone G.S., Thurber L.G., Proffen B.L., Ecklund K., et al. Bridge-Enhanced Anterior Cruciate Ligament Repair: Two-Year Results of a First-in-Human Study. Orthop. J. Sports Med. 2019;7:2325967118824356. doi: 10.1177/2325967118824356. - DOI - PMC - PubMed
-
- Bachmaier S., DiFelice G.S., Sonnery-Cottet B., Douoguih W.A., Smith P.A., Pace L.J., Ritter D., Wijdicks C.A. Treatment of Acute Proximal Anterior Cruciate Ligament Tears-Part 1: Gap Formation and Stabilization Potential of Repair Techniques. Orthop. J. Sports Med. 2020;8:2325967119897421. doi: 10.1177/2325967119897421. - DOI - PMC - PubMed
-
- Jonkergouw A., Van Der List J.P., DiFelice G.S. Arthroscopic primary repair of proximal anterior cruciate ligament tears: Outcomes of the first 56 consecutive patients and the role of additional internal bracing. Knee Surg. Sports Traumatol. Arthrosc. 2019;27:21–28. doi: 10.1007/s00167-018-5338-z. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
