

A Target for Increased Mortality Risk in Critically Ill Patients: The Concept of Perpetuity
- PMID: 34501419
- PMCID: PMC8432225
- DOI: 10.3390/jcm10173971
A Target for Increased Mortality Risk in Critically Ill Patients: The Concept of Perpetuity
Abstract
Background: Emergency medicine is acuity-based and focuses on time-sensitive treatments for life-threatening diseases. Prolonged time in the emergency department, however, is associated with higher mortality in critically ill patients. Thus, we explored management after an acuity-based intervention, which we call perpetuity, as a potential mechanism for increased risk. To explore this concept, we evaluated the impact of each hour above a lung-protective tidal volume on risk of mortality.
Methods: This cohort analysis includes all critically ill, non-trauma, adult patients admitted to two academic EDs between 1 November 2013 and 30 April 2017. Cox models with time-varying covariates were developed with time in perpetuity as a time-varying covariate, defined as hours above 8 mL/kg ideal body weight, adjusted for covariates. The primary outcome was the time to in-hospital death.
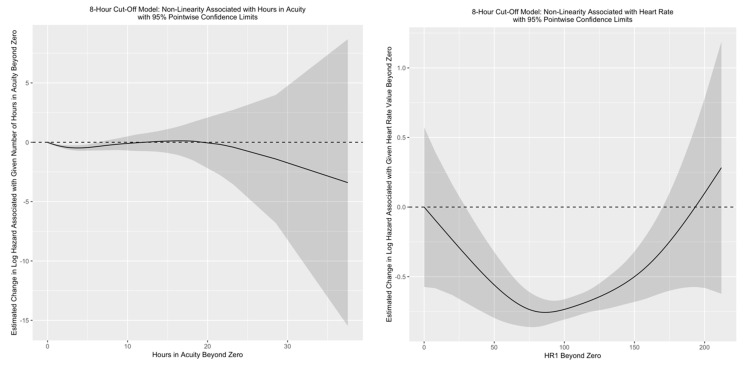
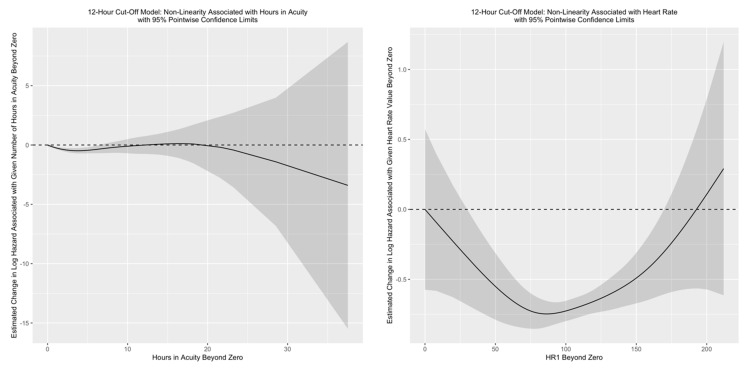
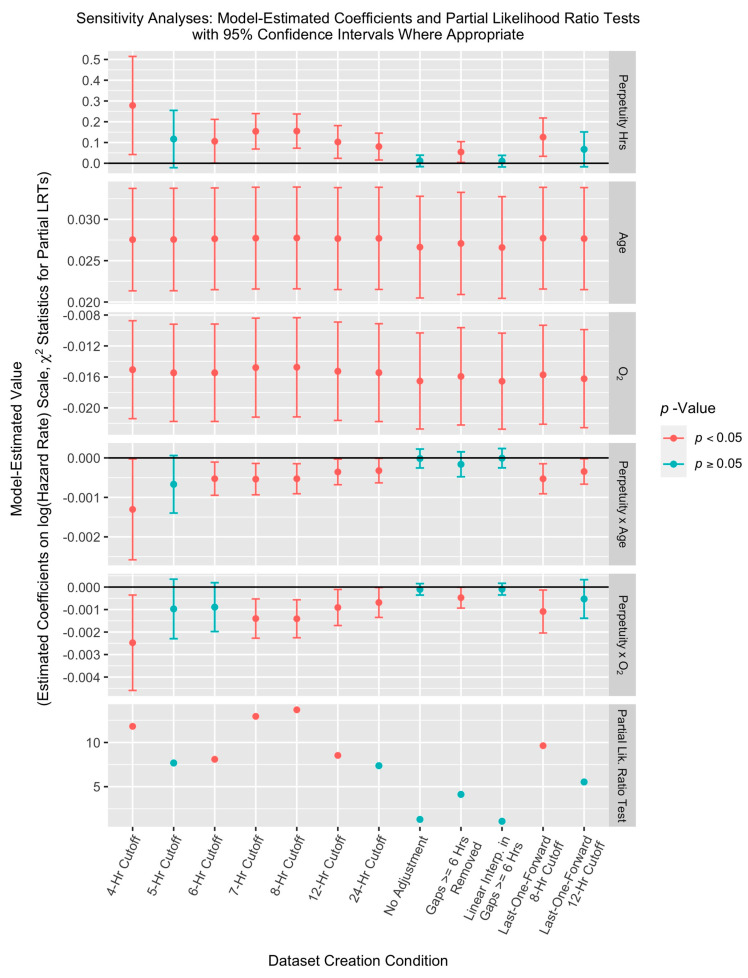
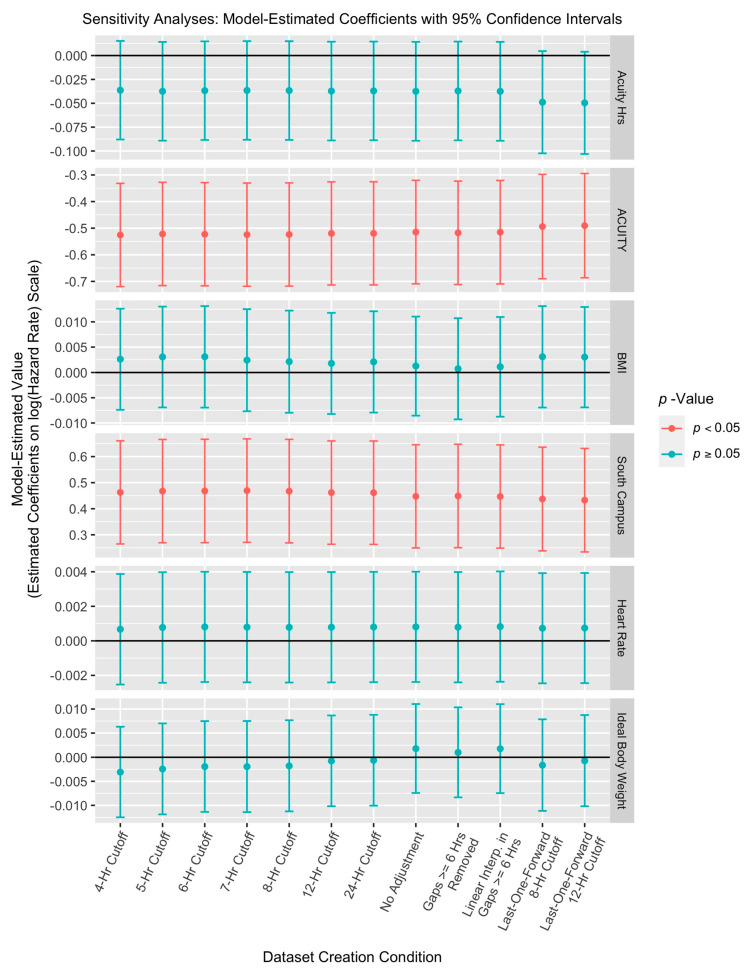
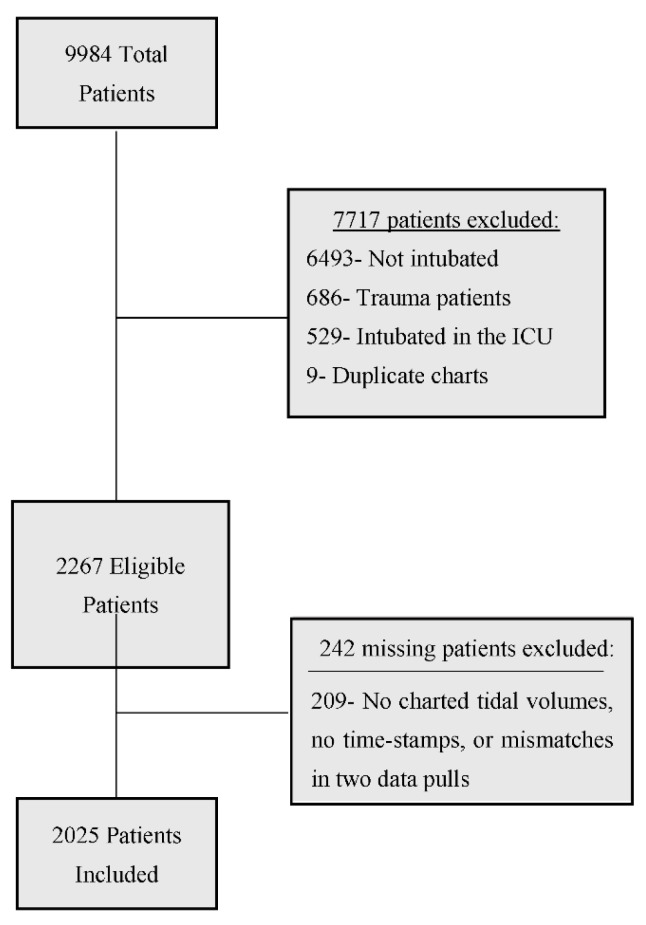
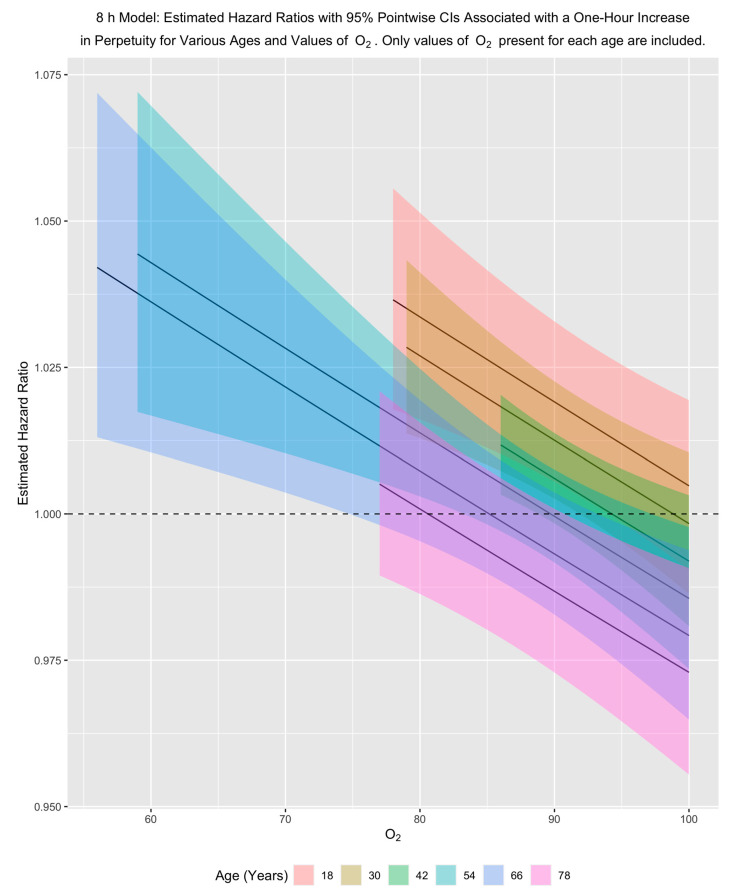
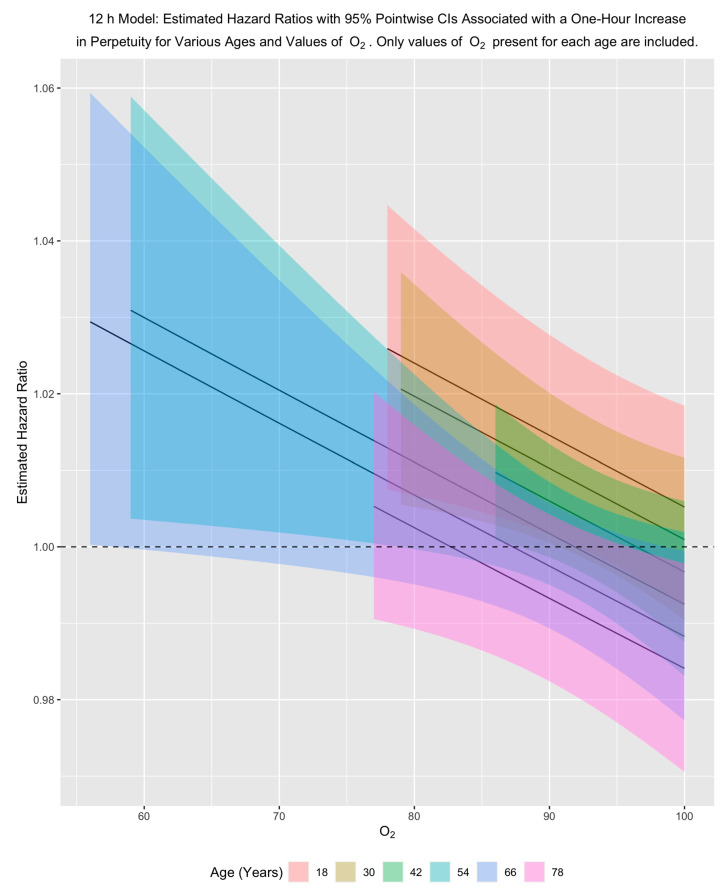
Results: Our analysis included 2025 patients, 321 (16%) of whom had at least 1 h of perpetuity time. A partial likelihood-ratio test comparing models with and without hours in perpetuity was statistically significant (χ2(3) = 13.83, p = 0.0031). There was an interaction between age and perpetuity (Relative risk (RR) 0.9995; 95% Confidence interval (CI95): 0.9991-0.9998). For example, for each hour above 8 mL/kg ideal body weight, a 20-year-old with 90% oxygen saturation has a relative risk of death of 1.02, but a 40-year-old with 90% oxygen saturation has a relative risk of 1.01.
Conclusions: Perpetuity, illustrated through the lens of mechanical ventilation, may represent a target for improving outcomes in critically ill patients, starting in the emergency department. Research is needed to evaluate the types of patients and interventions in which perpetuity plays a role.
Keywords: acuity; critical care; critically ill; emergency department; intubation; mechanical ventilation; perpetuity.
Conflict of interest statement
J.M.M. reports no conflict of interest; J.M.F. reports no conflict of interest; E.J.B. reports no conflict of interest; C.D.H. reports no conflict of interest; E.S.C. reports no conflict of interest; K.L. reports no conflict of interest; C.B.C. reports no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Control C.F.D. National Hospital Ambulatory Medical Care Survey: 2011 Emergency Department Summary Tables. [(accessed on 5 August 2021)]; Available online: http://www.cdc.gov/nchs/ahcd.htm.
-
- Rui P., Kang K., Ashman J.J. National Hospital Ambulatory Medical Care Survey: 2016 Emergency Department Summary Tables. [(accessed on 5 August 2021)];2016 Available online: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf.
-
- Medicine I.O. The National Academies of Sciences Engineering Medicine. The National Academies Press; Washington, DC, USA: 2006. Hospital-Based Emergency Care: At the Breaking Point.
LinkOut - more resources
Full Text Sources
Miscellaneous
