

Adverse Features of Rectourethral Fistula Requiring Extirpative Surgery and Permanent Dual Diversion: Our Experience and Recommendations
- PMID: 34501462
- PMCID: PMC8432514
- DOI: 10.3390/jcm10174014
Adverse Features of Rectourethral Fistula Requiring Extirpative Surgery and Permanent Dual Diversion: Our Experience and Recommendations
Abstract
Introduction: To report a series of men with a rectourethral fistula (RUF) resulting from pelvic cancer treatments and explore their therapeutic differences and impact on the functional outcomes and quality of life highlighting the adverse features that should determine permanent urinary or dual diversion.
Methods: A retrospective database search was performed in four centers to identify patients with RUF resulting from pelvic cancer treatment. Medical records were analyzed for the demographics, comorbidities, diagnostic evaluation, fistula characteristics, surgical approaches and outcomes. The endpoints analyzed included a successful fistula closure following a repair and the impact of the potential adverse features on outcomes.
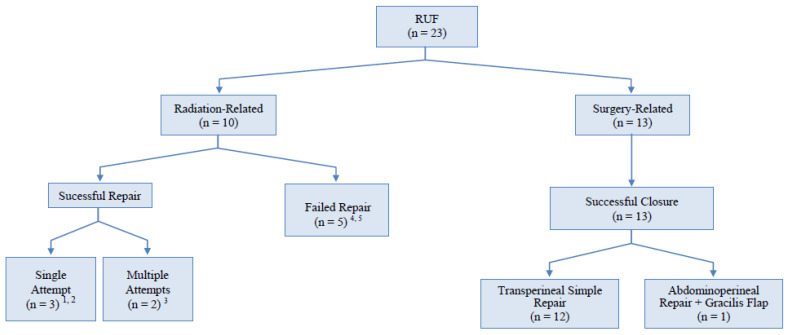
Results: Twenty-three patients, aged 57-79 years (median 68), underwent an RUF reconstruction. The median follow-up (FU) was 54 months (range 18-115). The patients were divided into two groups according to the etiology: radiation/energy-ablation treatments with or without surgery (G1, n = 10) and surgery only (G2, n = 13). All of the patients underwent a temporary diverting colostomy and suprapubic cystostomy. Overall, a successful RUF closure was achieved in 18 (78%) patients. An interposition flap was used in six (60%) patients and one (7.7%) patient in groups G1 and G2, respectively (p = 0.019). The RUF was managed successfully in all 13 patients in group G2 as opposed to 5/10 (50%) in group G1 (p = 0.008). The patients in the radiation/energy-ablation group were more likely to require permanent dual diversion (50% vs. 0%, p < 0.0075).
Conclusion: Radiation/energy-ablation therapies are associated with a more severe RUF and more complex reconstructions. Most of these patients require an abdominoperineal approach and flap interposition. The failure of an RUF repair with the need for permanent dual diversion, eventually combined with extirpative surgery, is higher after previous radiation/energy-ablation treatment. Therefore, permanent dual diversion as the primary treatment should always be included in the decision-making process as reconstruction may be futile in specific settings.
Keywords: pelvic cancer; prostate cancer; radiotherapy; reconstructive surgery; urinary fistula.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
