

Comparison of Respiratory Health Impacts Associated with Wood and Charcoal Biomass Fuels: A Population-Based Analysis of 475,000 Children from 30 Low- and Middle-Income Countries
- PMID: 34501907
- PMCID: PMC8431364
- DOI: 10.3390/ijerph18179305
Comparison of Respiratory Health Impacts Associated with Wood and Charcoal Biomass Fuels: A Population-Based Analysis of 475,000 Children from 30 Low- and Middle-Income Countries
Abstract
Background: The World Health Organisation reported that 45% of global acute respiratory infection (ARI) deaths in children under five years are attributable to household air pollution, which has been recognised to be strongly associated with solid biomass fuel usage in domestic settings. The introduction of legislative restrictions for charcoal production or purchase can result in unintended consequences, such as reversion to more polluting biomass fuels such as wood; which may increase health and environmental harms. However, there remains a paucity of evidence concerning the relative health risks between wood and charcoal. This study compares the risk of respiratory symptoms, ARI, and severe ARI among children aged under five years living in wood and charcoal fuel households across 30 low- and middle-income countries.
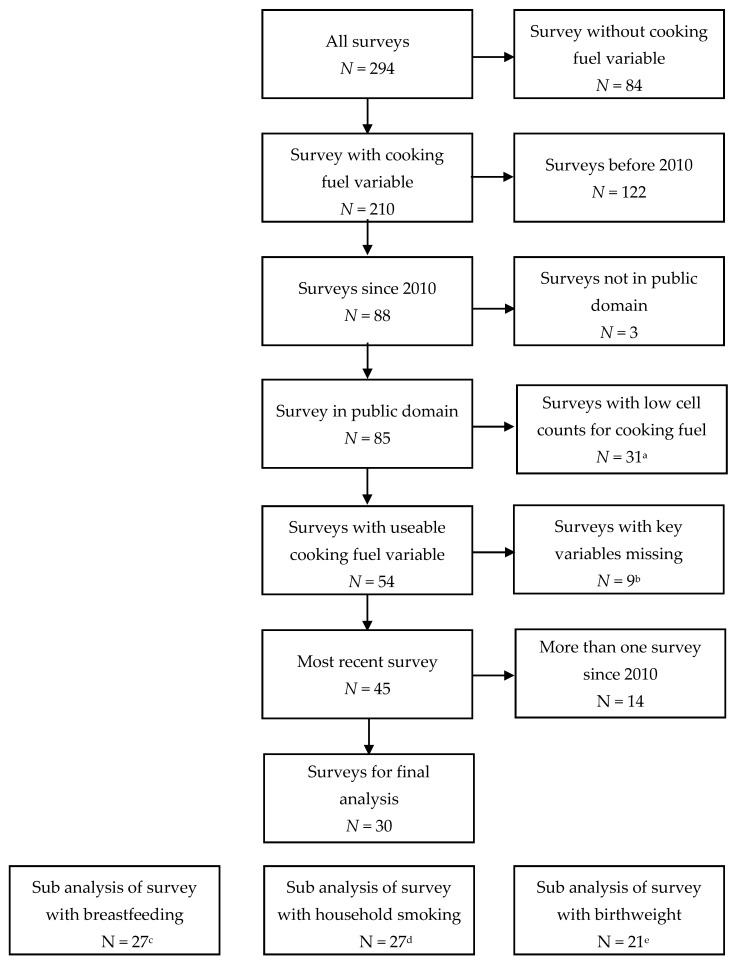
Methods: Data from children (N = 475,089) residing in wood or charcoal cooking households were extracted from multiple population-based Demographic and Health Survey databases (DHS) (N = 30 countries). Outcome measures were obtained from a maternal report of respiratory symptoms (cough, shortness of breath and fever) occurring in the two weeks prior to the survey date, generating a composite measure of ARI (cough and shortness of breath) and severe ARI (cough, shortness of breath and fever). Multivariable logistic regression analyses were implemented, with adjustment at individual, household, regional and country level for relevant demographic, social, and health-related confounding factors.
Results: Increased odds ratios of fever (AOR: 1.07; 95% CI: 1.02-1.12) were observed among children living in wood cooking households compared to the use of charcoal. However, no association was observed with shortness of breath (AOR: 1.03; 95% CI: 0.96-1.10), cough (AOR: 0.99; 95% CI: 0.95-1.04), ARI (AOR: 1.03; 95% CI: 0.96-1.11) or severe ARI (AOR: 1.07; 95% CI: 0.99-1.17). Within rural areas, only shortness of breath was observed to be associated with wood cooking (AOR: 1.08; 95% CI: 1.01-1.15). However, an increased odds ratio of ARI was observed in Asian (AOR: 1.25; 95% CI: 1.04-1.51) and East African countries (AOR: 1.11; 95% CI: 1.01-1.22) only.
Conclusion: Our population-based observational data indicates that in Asia and East Africa there is a greater risk of ARI among children aged under 5 years living in wood compared to charcoal cooking households. These findings have major implications for understanding the existing health impacts of wood-based biomass fuel usage and may be of relevance to settings where charcoal fuel restrictions are under consideration.
Keywords: acute respiratory infection; biomass fuel; household air pollution; low-and middle-income countries; respiratory symptoms.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures


References
-
- Cohen A.J., Brauer M., Burnett R., Anderson H.R., Frostad J., Estep K., Balakrishnan K., Brunekreef B., Dandona L., Dandona R., et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet. 2017;389:1907–1918. doi: 10.1016/S0140-6736(17)30505-6. - DOI - PMC - PubMed
-
- Smith K., Bruce N., Balakrishnan K., Adair-Rohani H., Balmes J., Chafe Z., Dherani M., Hosgood H.D., Mehta S., Pope D., et al. Millions dead: How do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. Annu. Rev. Public Health. 2014;35:185–206. doi: 10.1146/annurev-publhealth-032013-182356. - DOI - PubMed
-
- Gordon S.B., Bruce N.G., Grigg J., Hibberd P.L., Kurmi O.P., Lam K.H., Mortimer K., Asante K.P., Balakrishnan K., Balmes J., et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014;2:823–860. doi: 10.1016/S2213-2600(14)70168-7. - DOI - PMC - PubMed
-
- Tielsch J.M., Katz J., Thulasiraj R.D., Coles C.L., Sheeladevi S., Yanik E.L., Rahmathullah L. Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in south India. Int. J. Epidemiol. 2009;38:1351–1363. doi: 10.1093/ije/dyp286. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
