

Pediatric Catecholaminergic Polymorphic Ventricular Tachycardia: A Translational Perspective for the Clinician-Scientist
- PMID: 34502196
- PMCID: PMC8431429
- DOI: 10.3390/ijms22179293
Pediatric Catecholaminergic Polymorphic Ventricular Tachycardia: A Translational Perspective for the Clinician-Scientist
Abstract
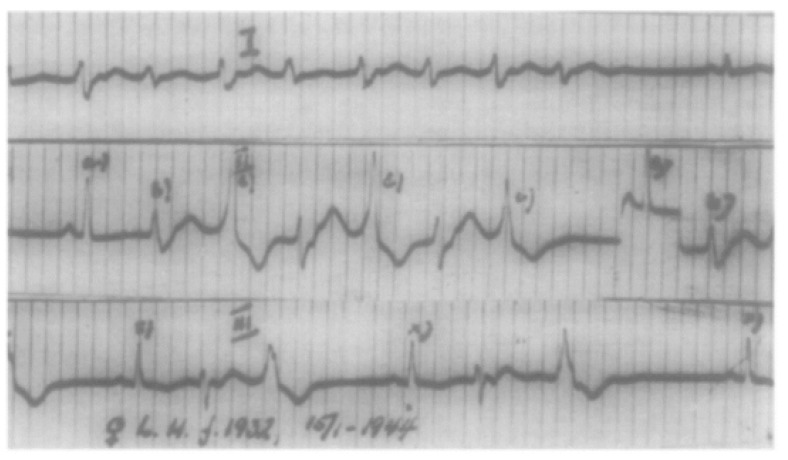
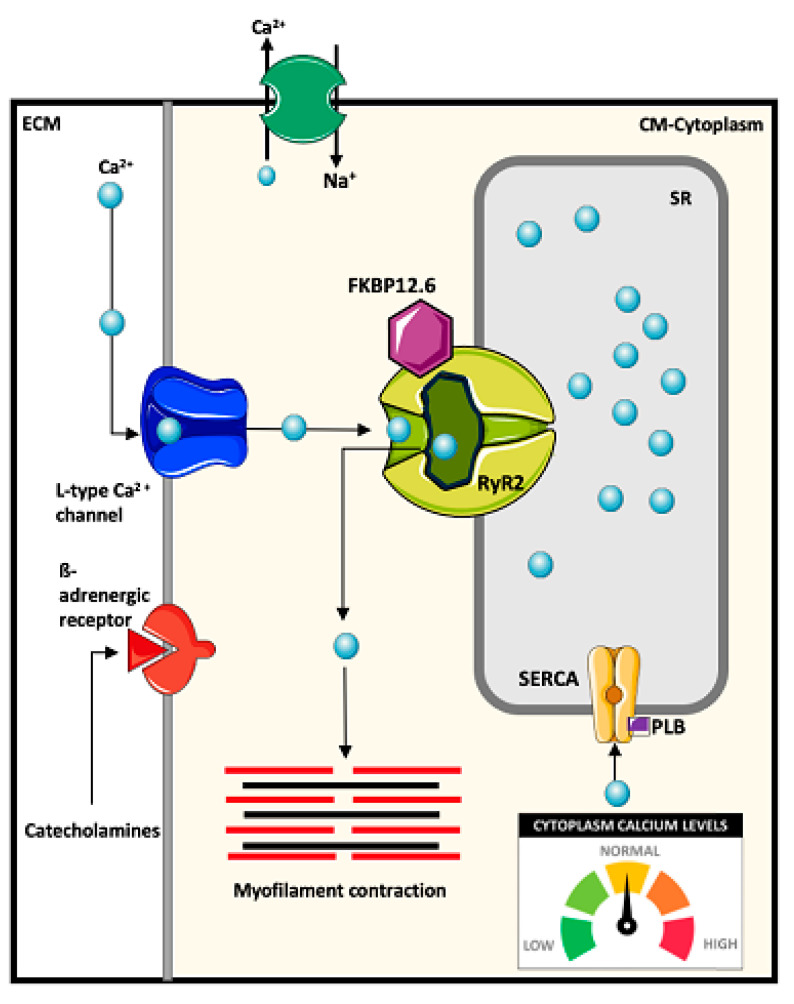
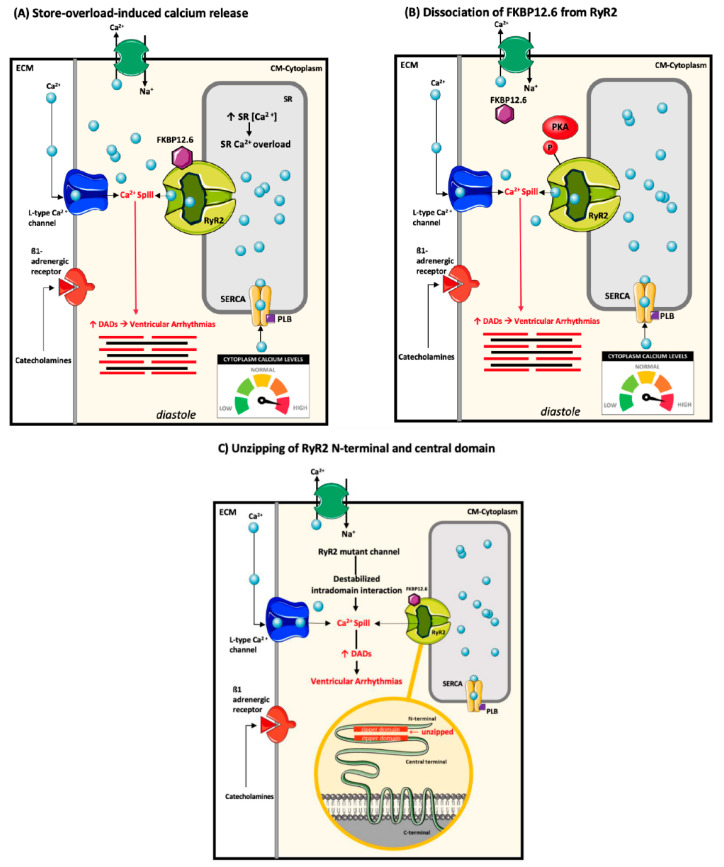
Catecholaminergic polymorphic ventricular tachycardia (CPVT) is a rare and potentially lethal inherited arrhythmia disease characterized by exercise or emotion-induced bidirectional or polymorphic ventricular tachyarrhythmias. The median age of disease onset is reported to be approximately 10 years of age. The majority of CPVT patients have pathogenic variants in the gene encoding the cardiac ryanodine receptor, or calsequestrin 2. These lead to mishandling of calcium in cardiomyocytes resulting in after-depolarizations, and ventricular arrhythmias. Disease severity is particularly pronounced in younger individuals who usually present with cardiac arrest and arrhythmic syncope. Risk stratification is imprecise and long-term prognosis on therapy is unknown despite decades of research focused on pediatric CPVT populations. The purpose of this review is to summarize contemporary data on pediatric CPVT, highlight knowledge gaps and present future research directions for the clinician-scientist to address.
Keywords: catecholaminergic polymorphic ventricular tachycardia; inherited arrhythmia; pediatric electrophysiology; primary electrical disease; ryanodine receptor; sudden cardiac death; ventricular tachycardia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Swan H., Piippo K., Viitasalo M., Heikkilä P., Paavonen T., Kainulainen K., Kere J., Keto P., Kontula K., Toivonen L. Arrhythmic disorder mapped to chromosome 1q42–q43 causes malignant polymorphic ventricular tachycardia in structurally normal hearts. J. Am. Coll. Cardiol. 1999;34:2035–2042. doi: 10.1016/S0735-1097(99)00461-1. - DOI - PubMed
-
- Priori S.G., Napolitano C., Memmi M., Colombi B., Drago F., Gasparini M., DeSimone L., Coltorti F., Bloise R., Keegan R., et al. Clinical and Molecular Characterization of Patients With Catecholaminergic Polymorphic Ventricular Tachycardia. Circulation. 2002;106:69–74. doi: 10.1161/01.CIR.0000020013.73106.D8. - DOI - PubMed
-
- Bauce B., Rampazzo A., Basso C., Bagattin A., Daliento L., Tiso N., Turrini P., Thiene G., Danieli G.A., Nava A. Screening for ryanodine receptor type 2 mutations in families with effort-induced polymorphic ventricular arrhythmias and sudden death. J. Am. Coll. Cardiol. 2002;40:341–349. doi: 10.1016/S0735-1097(02)01946-0. - DOI - PubMed
-
- Postma A.V., Denjoy I., Kamblock J., Alders M., Lupoglazoff J.-M., Vaksmann G., Dubosq-Bidot L., Sebillon P., Mannens M.M.A.M., Guicheney P., et al. Catecholaminergic polymorphic ventricular tachycardia: RYR2 mutations, bradycardia, and follow up of the patients. J. Med. Genet. 2005;42:863–870. doi: 10.1136/jmg.2004.028993. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
