

The Helicobacter pylori CagY Protein Drives Gastric Th1 and Th17 Inflammation and B Cell Proliferation in Gastric MALT Lymphoma
- PMID: 34502367
- PMCID: PMC8431018
- DOI: 10.3390/ijms22179459
The Helicobacter pylori CagY Protein Drives Gastric Th1 and Th17 Inflammation and B Cell Proliferation in Gastric MALT Lymphoma
Abstract
Background: the neoplastic B cells of the Helicobacter pylori-related low-grade gastric mucosa-associated lymphoid tissue (MALT) lymphoma proliferate in response to H. pylori, however, the nature of the H. pylori antigen responsible for proliferation is still unknown. The purpose of the study was to dissect whether CagY might be the H. pylori antigen able to drive B cell proliferation.
Methods: the B cells and the clonal progeny of T cells from the gastric mucosa of five patients with MALT lymphoma were compared with those of T cell clones obtained from five H. pylori-infected patients with chronic gastritis. The T cell clones were assessed for their specificity to H. pylori CagY, cytokine profile and helper function for B cell proliferation.
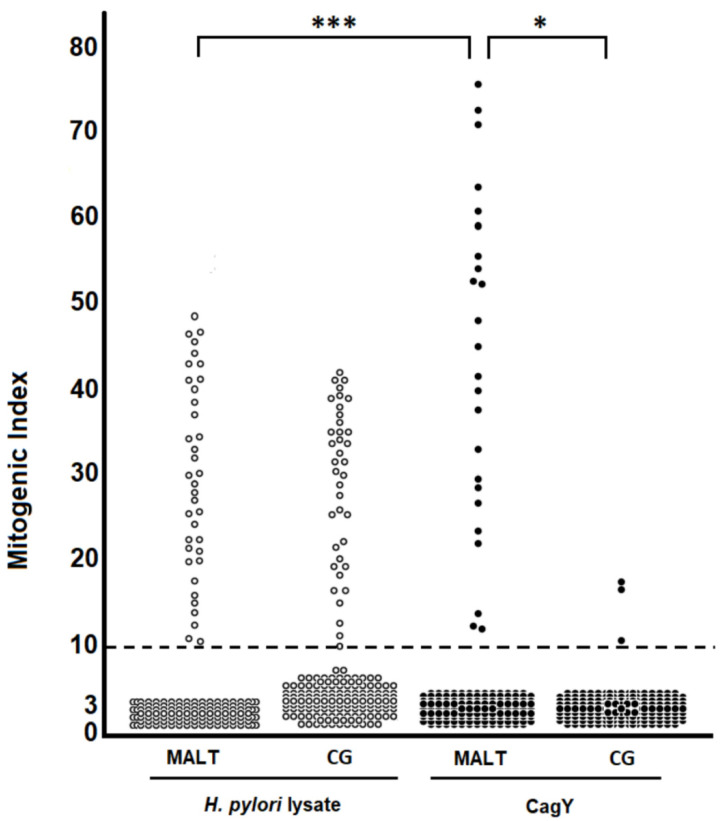
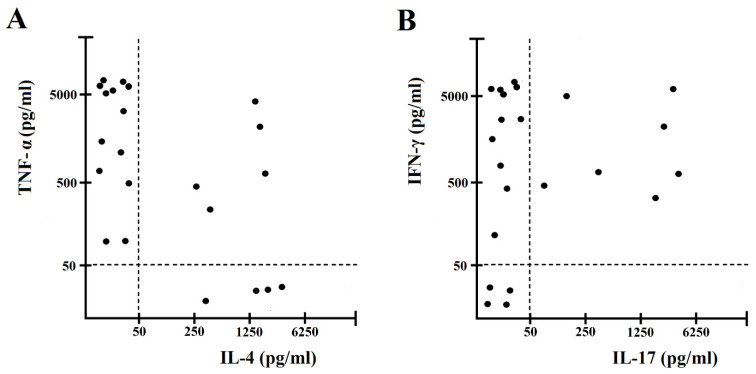
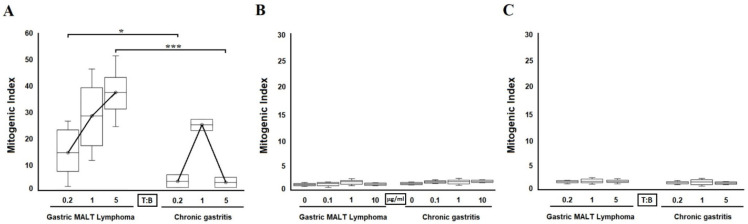
Results: 22 of 158 CD4+ (13.9%) gastric clones from MALT lymphoma and three of 179 CD4+ (1.7%) clones from chronic gastritis recognized CagY. CagY predominantly drives Interferon-gamma (IFN-γ) and Interleukin-17 (IL-17) secretion by gastric CD4+ T cells from H. pylori-infected patients with low-grade gastric MALT lymphoma. All MALT lymphoma-derived clones dose dependently increased their B cell help, whereas clones from chronic gastritis lost helper activity at T-to-B-cell ratios greater than 1.
Conclusion: the results obtained indicate that CagY drives both B cell proliferation and T cell activation in gastric MALT lymphomas.
Keywords: B cells; CagY; Helicobacter pylori; MALT; T cells; cytokines; gastric lymphoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pellicano R., Ribaldone D.G., Fagoonee S., Astegiano M., Saracco G.M., Mégraud F. A 2016 panorama of Helicobacter pylori infection: Key messages for clinicians. Panminerva Med. 2016;58:304–317. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
