

Factors Associated with Time to Conversion from Active Surveillance to Treatment for Prostate Cancer in a Multi-Institutional Cohort
- PMID: 34503355
- PMCID: PMC8734323
- DOI: 10.1097/JU.0000000000001937
Factors Associated with Time to Conversion from Active Surveillance to Treatment for Prostate Cancer in a Multi-Institutional Cohort
Abstract
Purpose: We examined the demographic and clinicopathological parameters associated with the time to convert from active surveillance to treatment among men with prostate cancer.
Materials and methods: A multi-institutional cohort of 7,279 patients managed with active surveillance had data and biospecimens collected for germline genetic analyses.
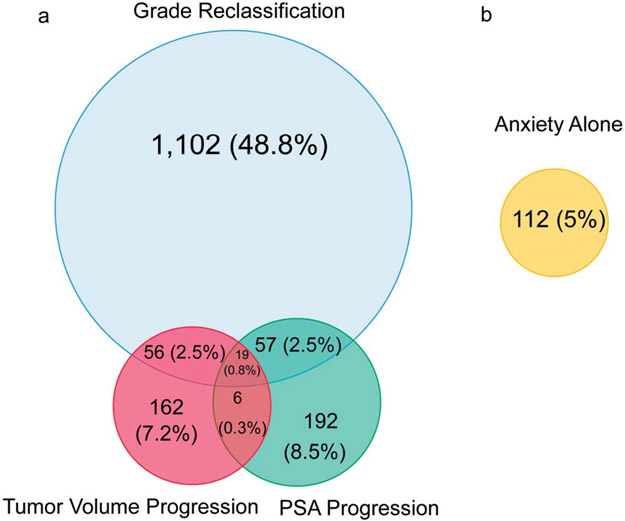
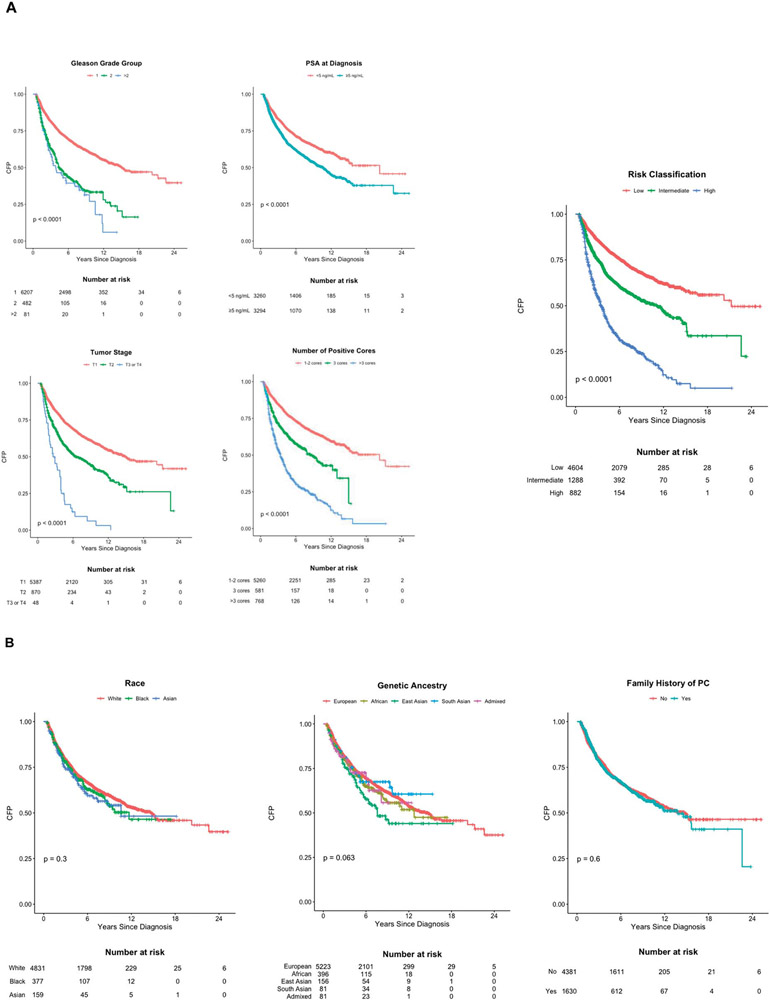
Results: Of 6,775 men included in the analysis, 2,260 (33.4%) converted to treatment at a median followup of 6.7 years. Earlier conversion was associated with higher Gleason grade groups (GG2 vs GG1 adjusted hazard ratio [aHR] 1.57, 95% CI 1.36-1.82; ≥GG3 vs GG1 aHR 1.77, 95% CI 1.29-2.43), serum prostate specific antigen concentrations (aHR per 5 ng/ml increment 1.18, 95% CI 1.11-1.25), tumor stages (cT2 vs cT1 aHR 1.58, 95% CI 1.41-1.77; ≥cT3 vs cT1 aHR 4.36, 95% CI 3.19-5.96) and number of cancerous biopsy cores (3 vs 1-2 cores aHR 1.59, 95% CI 1.37-1.84; ≥4 vs 1-2 cores aHR 3.29, 95% CI 2.94-3.69), and younger age (age continuous per 5-year increase aHR 0.96, 95% CI 0.93-0.99). Patients with high-volume GG1 tumors had a shorter interval to conversion than those with low-volume GG1 tumors and behaved like the higher-risk patients. We found no significant association between the time to conversion and self-reported race or genetic ancestry.
Conclusions: A shorter time to conversion from active surveillance to treatment was associated with higher-risk clinicopathological tumor features. Furthermore, patients with high-volume GG1 tumors behaved similarly to those with intermediate and high-risk tumors. An exploratory analysis of self-reported race and genetic ancestry revealed no association with the time to conversion.
Keywords: human genetics; prostatic neoplasms; race factors; watchful waiting.
Figures
Comment in
-
Editorial Comment.J Urol. 2021 Nov;206(5):1155-1156. doi: 10.1097/JU.0000000000001937.01. Epub 2021 Sep 10. J Urol. 2021. PMID: 34503356 No abstract available.
-
Urological Oncology: Prostate Cancer.J Urol. 2022 Sep;208(3):736-738. doi: 10.1097/JU.0000000000002796. Epub 2022 Jun 27. J Urol. 2022. PMID: 35757917 No abstract available.
References
-
- Sanda MG, Cadeddu JA, Kirkby E et al. : Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Part I: Risk stratification, shared decision making, and care options. J Urol 2018; 199: 683. - PubMed
-
- Bruinsma SM, Zhang L, Roobol MJ et al. : The Movember Foundation's GAP3 cohort: a profile of the largest global prostate cancer active surveillance database to date. BJU Int 2018; 121: 737. - PubMed
