

Development of weight and age-based dosing of daily primaquine for radical cure of vivax malaria
- PMID: 34503519
- PMCID: PMC8427859
- DOI: 10.1186/s12936-021-03886-w
Development of weight and age-based dosing of daily primaquine for radical cure of vivax malaria
Abstract
Background: In many endemic areas, Plasmodium vivax malaria is predominantly a disease of young adults and children. International recommendations for radical cure recommend fixed target doses of 0.25 or 0.5 mg/kg/day of primaquine for 14 days in glucose-6-phosphate dehydrogenase normal patients of all ages. However, for many anti-malarial drugs, including primaquine, there is evidence that children have lower exposures than adults for the same weight-adjusted dose. The aim of the study was to develop 14-day weight-based and age-based primaquine regimens against high-frequency relapsing tropical P. vivax.
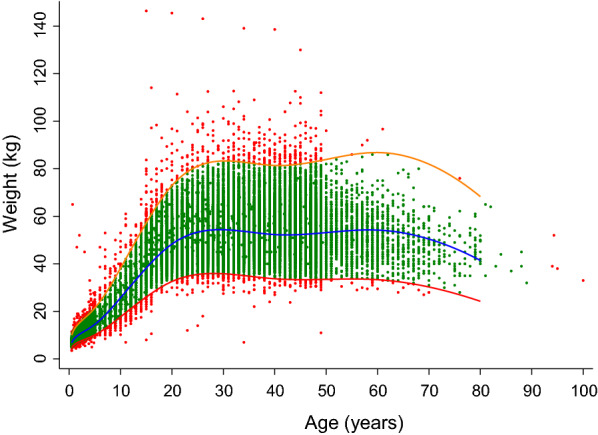
Methods: The recommended adult target dose of 0.5 mg/kg/day (30 mg in a 60 kg patient) is highly efficacious against tropical P. vivax and was assumed to produce optimal drug exposure. Primaquine doses were calculated using allometric scaling to derive a weight-based primaquine regimen over a weight range from 5 to 100 kg. Growth curves were constructed from an anthropometric database of 53,467 individuals from the Greater Mekong Subregion (GMS) to define weight-for-age relationships. The median age associated with each weight was used to derive an age-based dosing regimen from the weight-based regimen.
Results: The proposed weight-based regimen has 5 dosing bands: (i) 5-7 kg, 5 mg, resulting in 0.71-1.0 mg/kg/day; (ii) 8-16 kg, 7.5 mg, 0.47-0.94 mg/kg/day; (iii) 17-40 kg, 15 mg, 0.38-0.88 mg/kg/day; (iv) 41-80 kg, 30 mg, 0.37-0.73 mg/kg/day; and (v) 81-100 kg, 45 mg, 0.45-0.56 mg/kg/day. The corresponding age-based regimen had 4 dosing bands: 6-11 months, 5 mg, 0.43-1.0 mg/kg/day; (ii) 1-5 years, 7.5 mg, 0.35-1.25 mg/kg/day; (iii) 6-14 years, 15 mg, 0.30-1.36 mg/kg/day; and (iv) ≥ 15 years, 30 mg, 0.35-1.07 mg/kg/day.
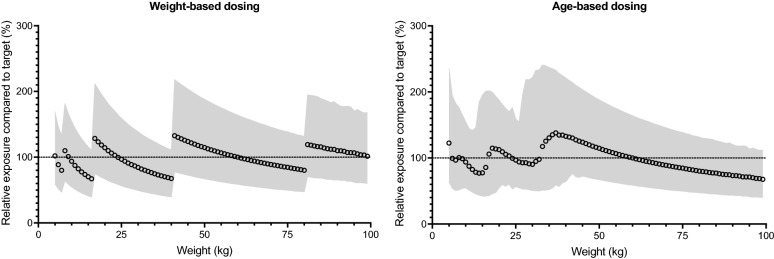
Conclusion: The proposed weight-based regimen showed less variability around the primaquine dose within each dosing band compared to the age-based regimen and is preferred. Increased dose accuracy could be achieved by additional dosing bands for both regimens. The age-based regimen might not be applicable to regions outside the GMS, which must be based on local anthropometric data. Pharmacokinetic data in small children are needed urgently to inform the proposed regimens.
Keywords: Age-based dosing; Allometric scaling; Plasmodium vivax; Primaquine; Weight-based dosing.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests. Philippe Buchy is currently an employee of GSK Vaccines in Singapore but his work is unrelated to this work.
Figures
References
-
- WHO . Guidelines for the treatment of malaria. 2. Geneva: World Health Organization; 2010. - PubMed
-
- WHO. Guidelines for the treatment of malaria, 3rd edn. Geneva: World Health Organization; 2015. WHO Guidelines Approved by the Guidelines Review Committee.
-
- Taylor WRJ, Thriemer K, von Seidlein L, Yuentrakul P, Assawariyathipat T, Assefa A, et al. Short-course primaquine for the radical cure of Plasmodium vivax malaria: a multicentre, randomised, placebo-controlled non-inferiority trial. Lancet. 2019;394:929–938. doi: 10.1016/S0140-6736(19)31285-1. - DOI - PMC - PubMed
-
- Chu CS, Phyo AP, Turner C, Win HH, Poe NP, Yotyingaphiram W, Thinraow S, et al. Chloroquine versus dihydroartemisinin-piperaquine with standard high-dose primaquine given either for 7 days or 14 days in Plasmodium vivax malaria. Clin Infect Dis. 2019;68:1311–1319. doi: 10.1093/cid/ciy735. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
