

High-Sensitivity C-Reactive Protein Modifies the Cardiovascular Risk of Lipoprotein(a): Multi-Ethnic Study of Atherosclerosis
- PMID: 34503676
- PMCID: PMC8444216
- DOI: 10.1016/j.jacc.2021.07.016
High-Sensitivity C-Reactive Protein Modifies the Cardiovascular Risk of Lipoprotein(a): Multi-Ethnic Study of Atherosclerosis
Abstract
Background: Little is known about the relationship between lipoprotein (a) [Lp(a)] and high-sensitivity C-reactive protein (hsCRP) and their joint association with atherosclerotic cardiovascular disease (ASCVD).
Objectives: The purpose of this study was to assess whether Lp(a)-associated ASCVD risk is modified by hsCRP in the context of primary prevention.
Methods: The current study included 4,679 participants from the MESA (Multi-Ethnic Study of Atherosclerosis) Apolipoprotein ancillary data set. Cox proportional hazards models and Kaplan-Meier curves were used to assess the association among Lp(a), hsCRP, and time to cardiovascular disease (CVD) events.
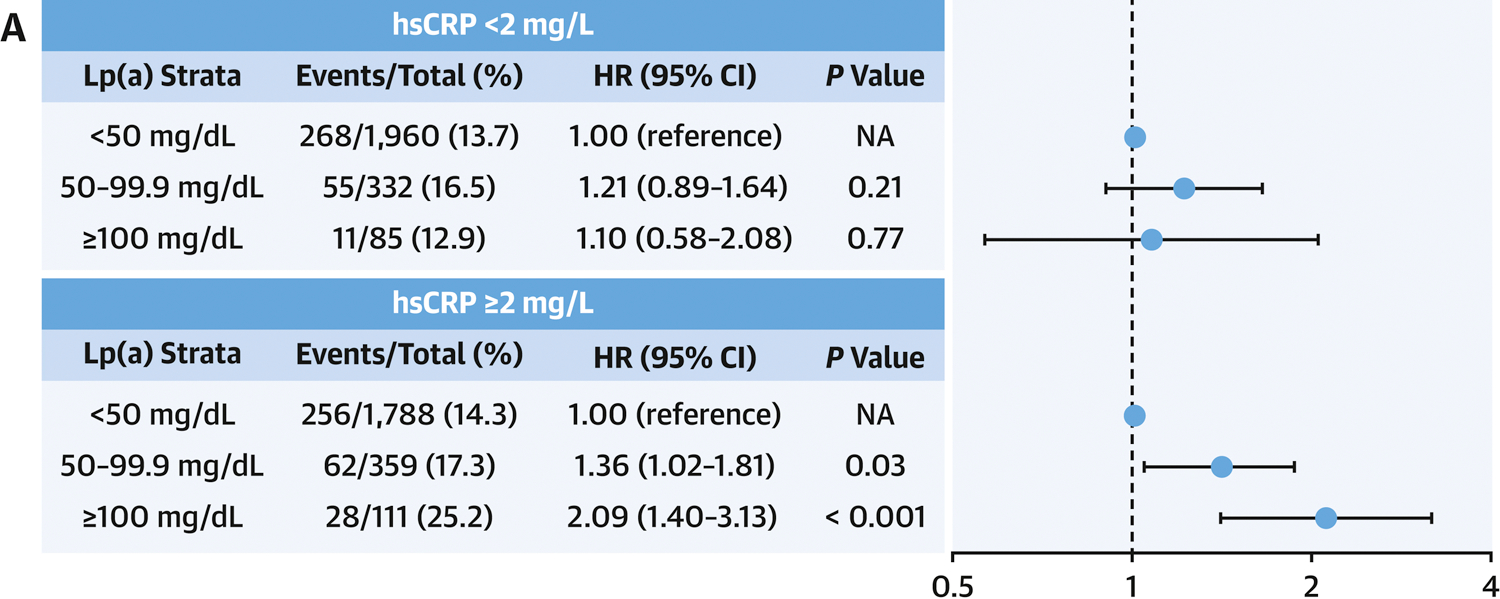
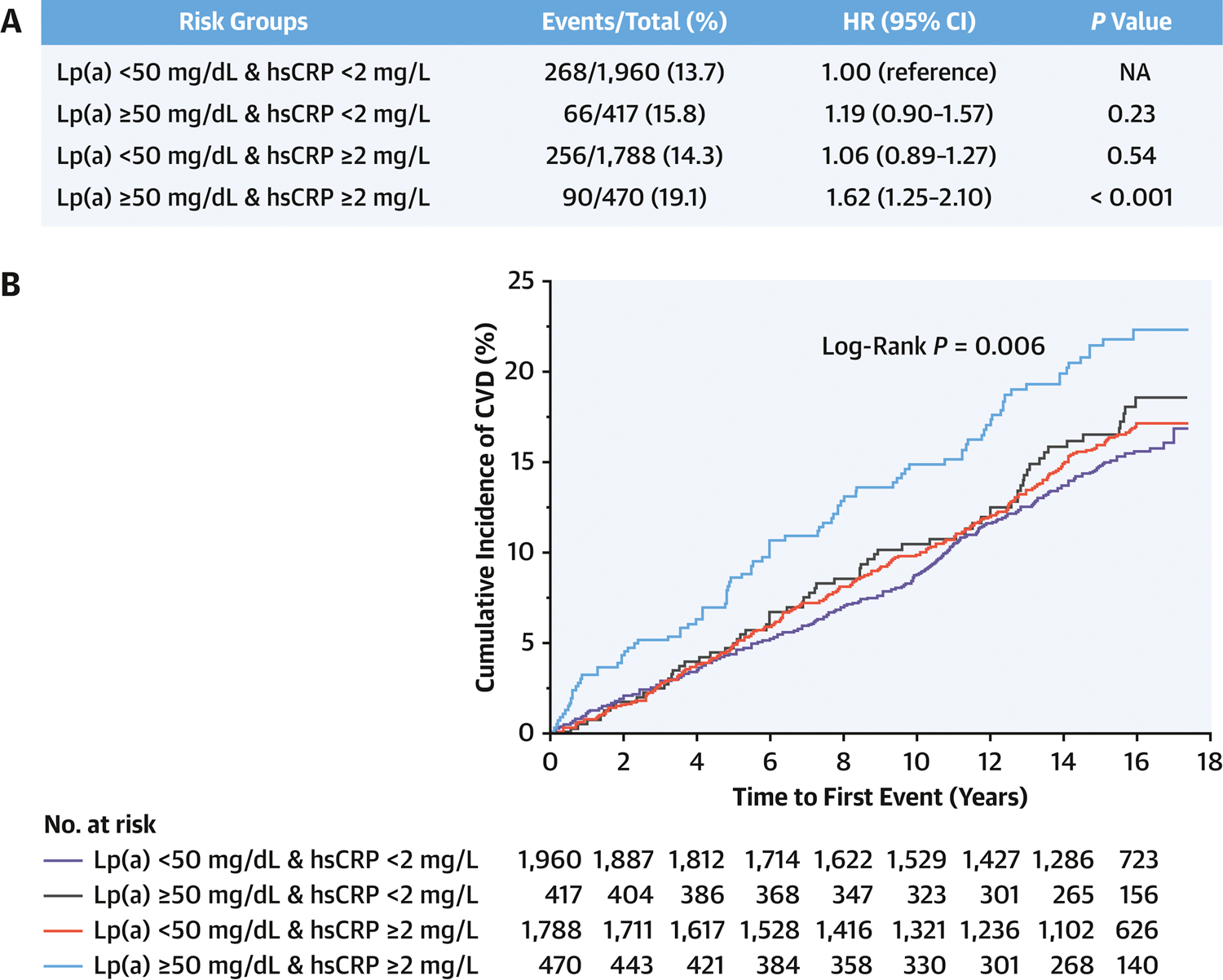
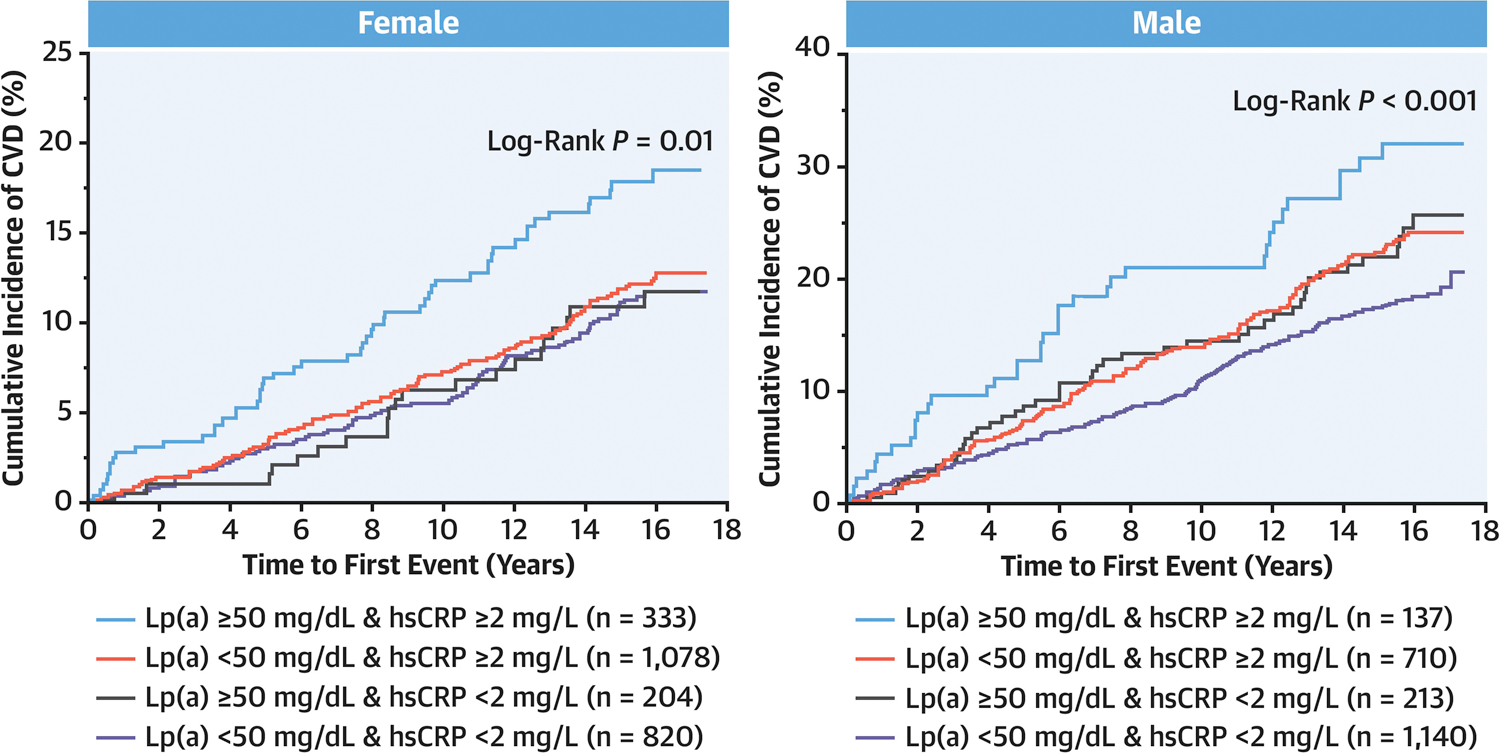
Results: During a mean follow-up of 13.6 years, 684 CVD events occurred. A significant interaction was observed between Lp(a) and hsCRP (P = 0.04). With hsCRP <2 mg/L, no significant CVD risk was observed at any level of Lp(a) from <50 mg/dL to >100 mg/dL. However, with hsCRP ≥2 mg/L, a significant CVD risk was observed with Lp(a) of 50-99.9 mg/dL (HR: 1.36; 95% CI: 1.02-1.81) and Lp(a) ≥100 mg/dL (HR: 2.09; 95% CI: 1.40-3.13). Isolated elevations of either Lp(a) or hsCRP were not associated with increased CVD risk. In contrast, the combination of elevated Lp(a) (≥50 mg/dL) and hsCRP (≥2 mg/L) was independently associated with significant CVD risk (HR: 1.62; 95% CI: 1.25-2.10) and all-cause mortality (HR: 1.39; 95% CI: 1.12-1.72).
Conclusions: Lp(a)-associated ASCVD risk is observed only with concomitant elevation of hsCRP. Individuals with concomitant presence of elevated Lp(a) and systemic inflammation have greater ASCVD risk and all-cause mortality, and thus may merit closer surveillance and more aggressive ASCVD risk management.
Keywords: ASCVD; Multi-Ethic Study of Atherosclerosis (MESA); cardiovascular risk; high-sensitivity C-reactive protein (hsCRP); inflammation; lipoprotein(a).
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures MESA is supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, and N01-HC-95169 from the National Heart, Lung, and Blood Institute; and by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from National Center for Advancing Translational Sciences. The MESA Air ancillary study was supported by a grant from the US Environmental Protection Agency’s Science to Achieve Results (STAR) program. Assistance Agreement number RD831697 awarded by the U.S. Environmental Protection to the University of Washington. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
Lifetime Risk Estimation in Atherosclerotic Cardiovascular Disease: Where Inflammation Meets Lipoprotein(a).J Am Coll Cardiol. 2021 Sep 14;78(11):1095-1096. doi: 10.1016/j.jacc.2021.07.035. J Am Coll Cardiol. 2021. PMID: 34503677 No abstract available.
References
-
- Benjamin EJ, Muntner P, Alonso A et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019;139:e56–e528. - PubMed
-
- Patel KV, Pandey A, de Lemos JA. Conceptual Framework for Addressing Residual Atherosclerotic Cardiovascular Disease Risk in the Era of Precision Medicine. Circulation 2018;137:2551–2553. - PubMed
-
- Mayr M, Gerszten R, Kiechl S. Cardiovascular Risk Beyond Low-Density Lipoprotein Cholesterol. J Am Coll Cardiol 2018;71:633–635. - PubMed
-
- Tsimikas S A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol 2017;69:692–711. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- KL2 TR001421/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- R01 HL111362/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
