

Exercise Intolerance in Older Adults With Heart Failure With Preserved Ejection Fraction: JACC State-of-the-Art Review
- PMID: 34503685
- PMCID: PMC8525886
- DOI: 10.1016/j.jacc.2021.07.014
Exercise Intolerance in Older Adults With Heart Failure With Preserved Ejection Fraction: JACC State-of-the-Art Review
Abstract
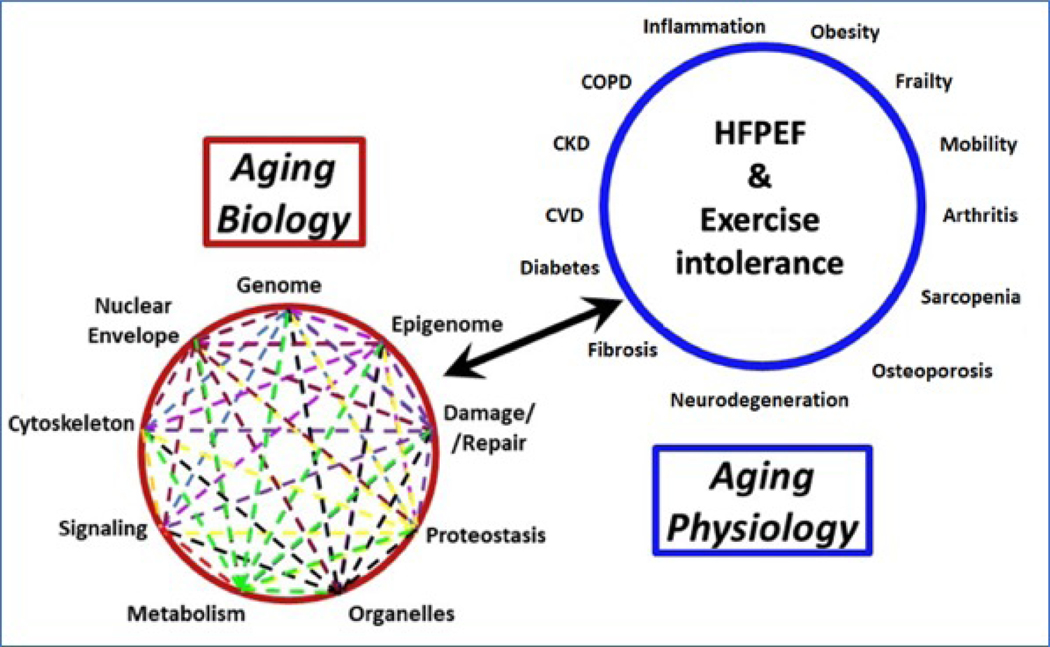
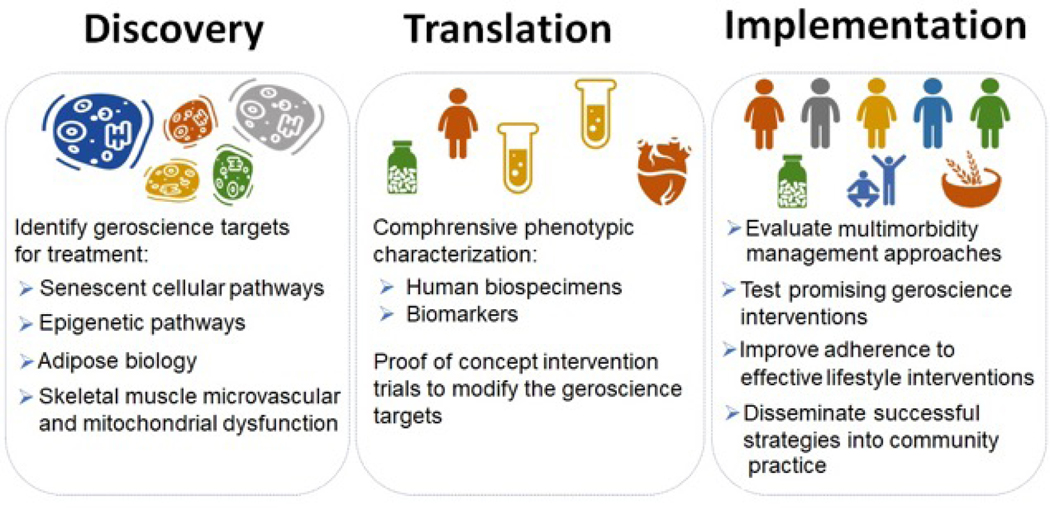
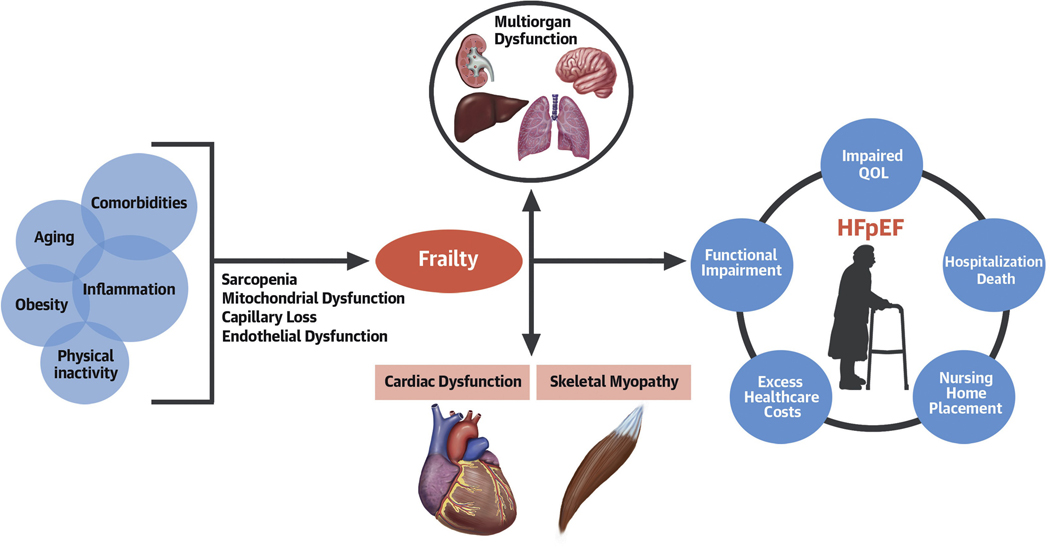
Exercise intolerance (EI) is the primary manifestation of chronic heart failure with preserved ejection fraction (HFpEF), the most common form of heart failure among older individuals. The recent recognition that HFpEF is likely a systemic, multiorgan disorder that shares characteristics with other common, difficult-to-treat, aging-related disorders suggests that novel insights may be gained from combining knowledge and concepts from aging and cardiovascular disease disciplines. This state-of-the-art review is based on the outcomes of a National Institute of Aging-sponsored working group meeting on aging and EI in HFpEF. We discuss aging-related and extracardiac contributors to EI in HFpEF and provide the rationale for a transdisciplinary, "gero-centric" approach to advance our understanding of EI in HFpEF and identify promising new therapeutic targets. We also provide a framework for prioritizing future research, including developing a uniform, comprehensive approach to phenotypic characterization of HFpEF, elucidating key geroscience targets for treatment, and conducting proof-of-concept trials to modify these targets.
Keywords: aging; exercise intolerance; heart failure with preserved ejection fraction; senescence; skeletal muscle.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The workshop “A Gero-centric Approach to Exercise Intolerance and Heart Failure with Preserved Ejection Fraction (HFpEF) in Older Adults: Elucidating and Targeting Extra-cardiac Contributors” was funded by the National Institute on Aging. The contents of this paper are solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH). Dr Pandey is supported by the Texas Health Resources Clinical Scholarship, the Gilead Sciences Research Scholar Program, the National Institute of Aging GEMSSTAR Grant (1R03AG067960-01), and Applied Therapeutics; has served on the advisory board for Roche Diagnostics; and has received nonfinancial support from Pfizer and Merck. Dr Butler has served as a consultant for Abbott, Adrenomed, Arena Pharma, Array, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Cardior, CVRx, Eli Lilly, G3 Pharma, Imbria, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, Novo Nordisk, Relypsa, Roche, Sequana Medical, V-Wave Limited, and Vifor. Dr Kellogg Jr is supported by NIH grants P30 AG044271 and K01AG059837. Dr Mentz has received research support and honoraria from Abbott, American Regent, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim/Eli Lilly, Boston Scientific, Cytokinetics, Fast BioMedical, Gilead, Medtronic, Merck, Novartis, Roche, Sanofi, and Vifor. Dr Forman is funded by NIH grants R01AG060499, R01AG058883, R01AG051376, and P30AG024827. Dr Borlaug is funded by NIH grant RO1 HL128526. Dr Simon has received grant support from Aadi; and has served as a consultant for Acceleron, Actelion, and United Therapeutics. Dr Chirinos is supported by NIH grants R01-HL 121510, R33-HL-146390, R01-AG058969, 1R01-HL104106, P01-HL094307, R03-HL146874, R56-HL136730, and 1R01HL153646-01; has served as a consultant for Bayer, Sanifit, Fukuda-Denshi, Bristol Myers Squibb, Johnson & Johnson, Edwards Lifesciences, Merck, and the Galway-Mayo Institute of Technology; is named as inventor in a University of Pennsylvania patent for the use of inorganic nitrates/nitrites for the treatment of heart failure and preserved ejection fraction; has received University of Pennsylvania research grants from National Institutes of Health, Fukuda-Denshi, Bristol Myers Squibb, Microsoft, and Abbott; has received payments for editorial roles from the American Heart Association, the American College of Cardiology, and Wiley; and has received research device loans from Atcor Medical, Fukuda-Denshi, Uscom, NDD Medical Technologies, Microsoft, and MicroVision Medical. Dr Sam is supported by NIH grant R01HL145985. Dr Molina is supported by NIH grant R21 AG051077. Dr Pipinos is supported by R01AG062198. Dr Lewis has received research funding from the National Institutes of Health R01-HL 151841, R01-HL131029, American Heart Association 15GPSGC-24800006, and Amgen, Cytokinetics, Applied Therapeutics, AstraZeneca, and Sonivie in relation to projects that are distinct from this work; has received honoraria outside of the current study from Pfizer, Merck, Boehringer Ingelheim, Novartis, American Regent, Cyclerion, Cytokinetics, and Amgen; and receives royalties from UpToDate for scientific content authorship related to exercise physiology. Dr Bertoni is partially supported by NIH grant 1R01HL127028-01; and has consulted with Premier/Merck on a diabetes quality improvement project. Dr Justice has received support from NIH grants K01AG059837 and P30AG021332. Dr Hummel is supported by NIH grants R01AG062582 and R01HL139813, and by VA grant I01CX001636. Dr Kitzman is supported in part by NIH grants R01AG18915, R01AG045551, P30AG021332, and U24AG059624, and by the Kermit G. Phillips Endowed Chair in Cardiovascular Medicine; has received honoraria outside the present study as a consultant for AbbVie, Bayer, Merck, Medtronic, Relypsa, Merck, Corvia Medical, Boehringer Ingelheim, Novo Nordisk, AstraZeneca, and Novartis; has received grant funding outside the present study from Novartis, Bayer, Novo Nordisk, and AstraZeneca; and has stock ownership in Gilead Sciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Kitzman DW, Gardin JM, Gottdiener JS et al. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol 2001;87:413–9. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG058659/AG/NIA NIH HHS/United States
- R03 HL146874/HL/NHLBI NIH HHS/United States
- R01 AG060499/AG/NIA NIH HHS/United States
- R01 HL104106/HL/NHLBI NIH HHS/United States
- U24 AG059624/AG/NIA NIH HHS/United States
- R01 AG062582/AG/NIA NIH HHS/United States
- R56 HL136730/HL/NHLBI NIH HHS/United States
- R01 AG058969/AG/NIA NIH HHS/United States
- R01 HL151841/HL/NHLBI NIH HHS/United States
- R33 HL146390/HL/NHLBI NIH HHS/United States
- K01 AG059837/AG/NIA NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- R21 AG051077/AG/NIA NIH HHS/United States
- R01 AG058883/AG/NIA NIH HHS/United States
- R01 HL145985/HL/NHLBI NIH HHS/United States
- R01 HL153646/HL/NHLBI NIH HHS/United States
- R01 HL128526/HL/NHLBI NIH HHS/United States
- R01 AG062198/AG/NIA NIH HHS/United States
- P01 HL094307/HL/NHLBI NIH HHS/United States
- R03 AG067960/AG/NIA NIH HHS/United States
- R01 HL127028/HL/NHLBI NIH HHS/United States
- R01 AG018915/AG/NIA NIH HHS/United States
- K24 AG070459/AG/NIA NIH HHS/United States
- R01 HL107577/HL/NHLBI NIH HHS/United States
- R01 HL139813/HL/NHLBI NIH HHS/United States
- I01 CX001636/CX/CSRD VA/United States
- R01 HL121510/HL/NHLBI NIH HHS/United States
- R01 AG062624/AG/NIA NIH HHS/United States
- P30 AG044271/AG/NIA NIH HHS/United States
- R01 AG045551/AG/NIA NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- R01 HL131029/HL/NHLBI NIH HHS/United States
