

Emergence of bedaquiline resistance in a high tuberculosis burden country
- PMID: 34503982
- PMCID: PMC8943268
- DOI: 10.1183/13993003.00621-2021
Emergence of bedaquiline resistance in a high tuberculosis burden country
Abstract
Rationale: Bedaquiline has been classified as a group A drug for the treatment of multidrug-resistant tuberculosis (MDR-TB) by the World Health Organization; however, globally emerging resistance threatens the effectivity of novel MDR-TB treatment regimens.
Objectives: We analysed pre-existing and emerging bedaquiline resistance in bedaquiline-based MDR-TB therapies, and risk factors associated with treatment failure and death.
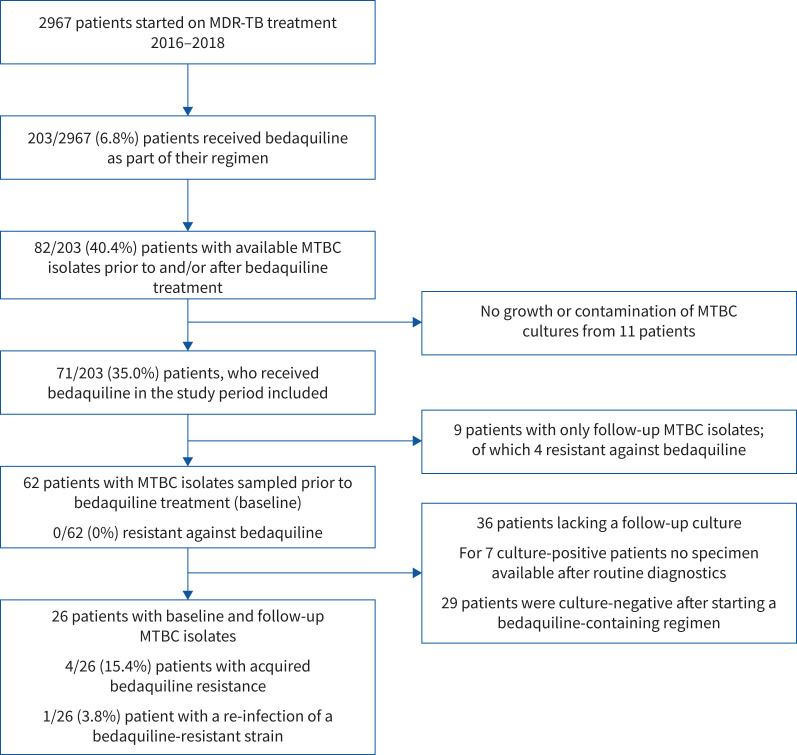
Methods: In a cross-sectional cohort study, we employed patient data, whole-genome sequencing (WGS) and phenotyping of Mycobacterium tuberculosis complex (MTBC) isolates. We could retrieve baseline isolates from 30.5% (62 out of 203) of all MDR-TB patients who received bedaquiline between 2016 and 2018 in the Republic of Moldova. This includes 26 patients for whom we could also retrieve a follow-up isolate.
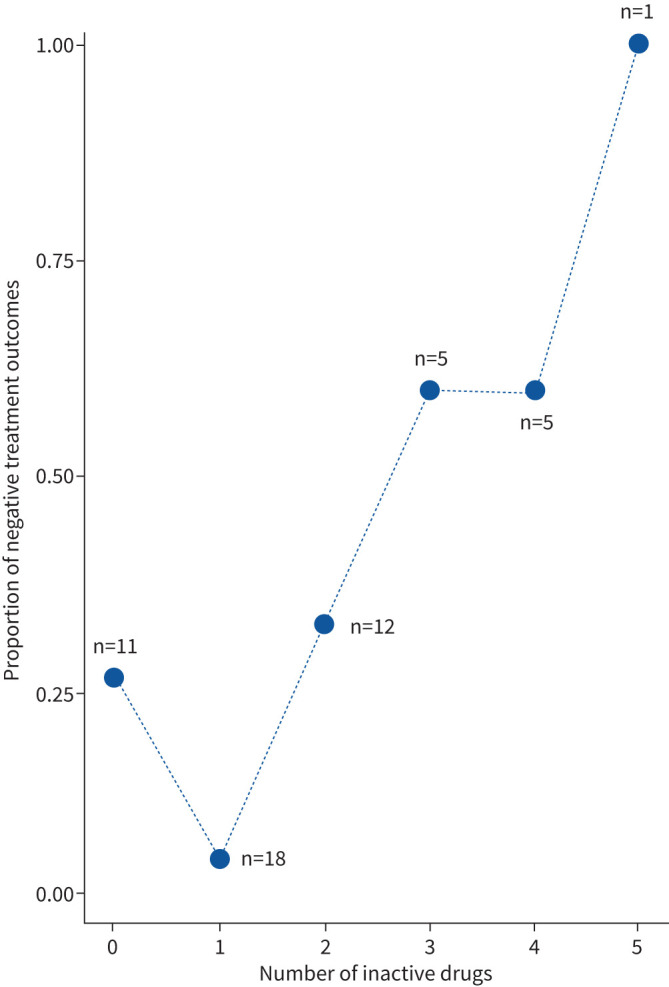
Measurements and main results: At baseline, all MTBC isolates were susceptible to bedaquiline. Among 26 patients with available baseline and follow-up isolates, four (15.3%) patients harboured strains which acquired bedaquiline resistance under therapy, while one (3.8%) patient was re-infected with a second bedaquiline-resistant strain. Treatment failure and death were associated with cavitary disease (p=0.011), and any additional drug prescribed in the bedaquiline-containing regimen with WGS-predicted resistance at baseline (OR 1.92 per unit increase, 95% CI 1.15-3.21; p=0.012).
Conclusions: MDR-TB treatments based on bedaquiline require a functional background regimen to achieve high cure rates and to prevent the evolution of bedaquiline resistance. Novel MDR-TB therapies with bedaquiline require timely and comprehensive drug resistance monitoring.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: E. Chesov has nothing to disclose. Conflict of interest: D. Chesov has nothing to disclose. Conflict of interest: F.P. Maurer has nothing to disclose. Conflict of interest: S. Andres has nothing to disclose. Conflict of interest: C. Utpatel has nothing to disclose. Conflict of interest: I. Barilar has nothing to disclose. Conflict of interest: A. Donica has nothing to disclose. Conflict of interest: M. Reimann has nothing to disclose. Conflict of interest: S. Niemann reports grants from EXC 2167 Precision Medicine in Inflammation, grants from Leibniz Science Campus Evolutionary Medicine of the LUNG, grants from German Center for Infection Research, during the conduct of the study. Conflict of interest: C. Lange reports personal fees from Chiesi, Gilead, Janssen, Novartis, Oxfordimmunotec and Insmed, outside the submitted work. Conflict of interest: V. Crudu has nothing to disclose. Conflict of interest: J. Heyckendorf has nothing to disclose. Conflict of interest: M. Merker has nothing to disclose.
Figures
Comment in
-
Guiding pragmatic treatment choices for rifampicin-resistant tuberculosis in the absence of second-line drug susceptibility testing.Eur Respir J. 2023 Nov 29;62(5):2300969. doi: 10.1183/13993003.00969-2023. Print 2023 Nov. Eur Respir J. 2023. PMID: 37945035 No abstract available.
References
-
- World Health Organization (WHO) . Global Tuberculosis Report 2020. Available from: www.who.int/tb/publications/global_report/en/ Date last accessed: 23 October 2020.
-
- World Health Organization (WHO) . WHO Consolidated Guidelines on Tuberculosis. Module 4: Treatment – Drug-Resistant Tuberculosis Treatment. https://apps.who.int/iris/bitstream/handle/10665/332397/9789240007048-en... Date last accessed: 7 July 2021. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical