

Prognostic role of Ki-67 in glioblastomas excluding contribution from non-neoplastic cells
- PMID: 34504133
- PMCID: PMC8429554
- DOI: 10.1038/s41598-021-95958-9
Prognostic role of Ki-67 in glioblastomas excluding contribution from non-neoplastic cells
Abstract
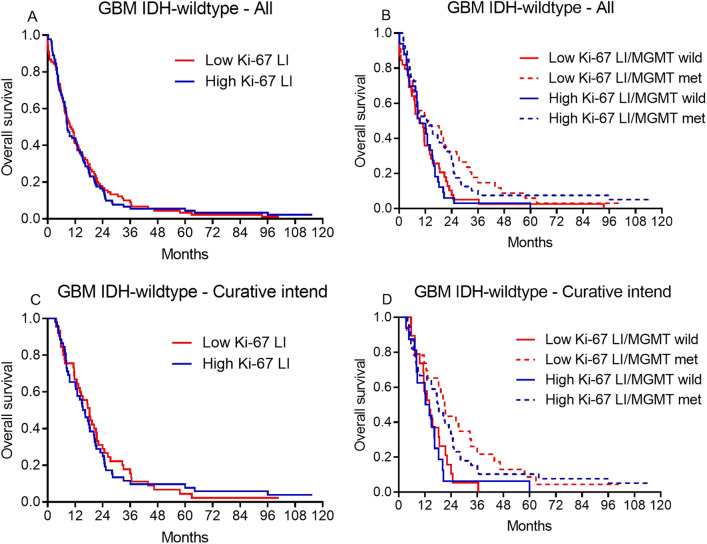
Survival of glioblastoma patients varies and prognostic markers are important in the clinical setting. With digital pathology and improved immunohistochemical multiplexing becoming a part of daily diagnostics, we investigated the prognostic value of the Ki-67 labelling index (LI) in glioblastomas more precisely than previously by excluding proliferation in non-tumor cells from the analysis. We investigated the Ki-67 LI in a well-annotated population-based glioblastoma patient cohort (178 IDH-wildtype, 3 IDH-mutated). Ki-67 was identified in full tumor sections with automated digital image analysis and the contribution from non-tumor cells was excluded using quantitative double-immunohistochemistry. For comparison of the Ki-67 LI between WHO grades (II-IV), 9 IDH-mutated diffuse astrocytomas and 9 IDH-mutated anaplastic astrocytomas were stained. Median Ki-67 LI increased with increasing WHO grade (median 2.7%, 6.4% and 27.5%). There was no difference in median Ki-67 LI between IDH-mutated and IDH-wildtype glioblastomas (p = 0.9) and Ki-67 LI was not associated with survival in glioblastomas in neither univariate (p = 0.9) nor multivariate analysis including MGMT promoter methylation status and excluding IDH-mutated glioblastomas (p = 0.2). Ki-67 may be of value in the differential diagnostic setting, but it must not be over-interpreted in the clinico-pathological context.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
