

Artificial intelligence sepsis prediction algorithm learns to say "I don't know"
- PMID: 34504260
- PMCID: PMC8429719
- DOI: 10.1038/s41746-021-00504-6
Artificial intelligence sepsis prediction algorithm learns to say "I don't know"
Abstract
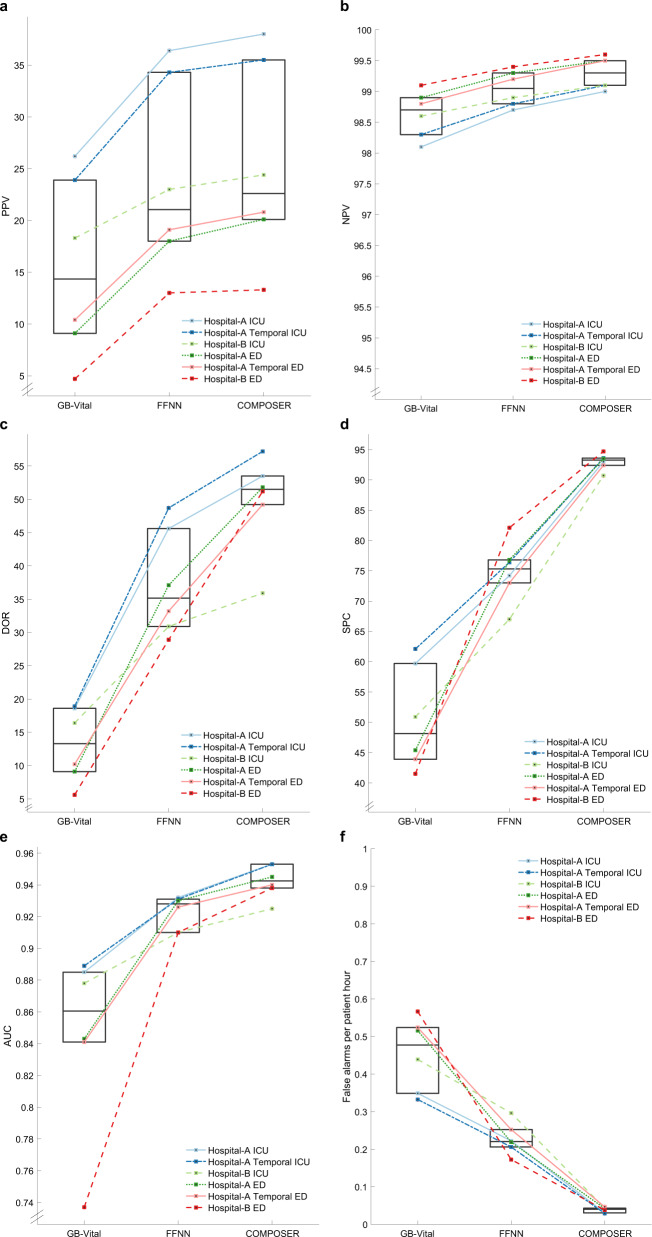
Sepsis is a leading cause of morbidity and mortality worldwide. Early identification of sepsis is important as it allows timely administration of potentially life-saving resuscitation and antimicrobial therapy. We present COMPOSER (COnformal Multidimensional Prediction Of SEpsis Risk), a deep learning model for the early prediction of sepsis, specifically designed to reduce false alarms by detecting unfamiliar patients/situations arising from erroneous data, missingness, distributional shift and data drifts. COMPOSER flags these unfamiliar cases as indeterminate rather than making spurious predictions. Six patient cohorts (515,720 patients) curated from two healthcare systems in the United States across intensive care units (ICU) and emergency departments (ED) were used to train and externally and temporally validate this model. In a sequential prediction setting, COMPOSER achieved a consistently high area under the curve (AUC) (ICU: 0.925-0.953; ED: 0.938-0.945). Out of over 6 million prediction windows roughly 20% and 8% were identified as indeterminate amongst non-septic and septic patients, respectively. COMPOSER provided early warning within a clinically actionable timeframe (ICU: 12.2 [3.2 22.8] and ED: 2.1 [0.8 4.5] hours prior to first antibiotics order) across all six cohorts, thus allowing for identification and prioritization of patients at high risk for sepsis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Centers for Medicare & Medicaid Services. QualityNet—inpatient hospitals specifications manual. Quality website. https://www.qualitynet.org/inpatient/specifications-manuals. Accessed August, 2020.
Grants and funding
- R35 GM143121/GM/NIGMS NIH HHS/United States
- R56 LM013517/LM/NLM NIH HHS/United States
- GBMF9052/Gordon and Betty Moore Foundation (Gordon E. and Betty I. Moore Foundation)
- R56LM013517/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- HHSO100201900015C/U.S. Department of Health & Human Services | Biomedical Advanced Research and Development Authority (BARDA)
