

Circulating EGFL7 distinguishes between IUGR and PE: an observational case-control study
- PMID: 34504270
- PMCID: PMC8429426
- DOI: 10.1038/s41598-021-97482-2
Circulating EGFL7 distinguishes between IUGR and PE: an observational case-control study
Abstract
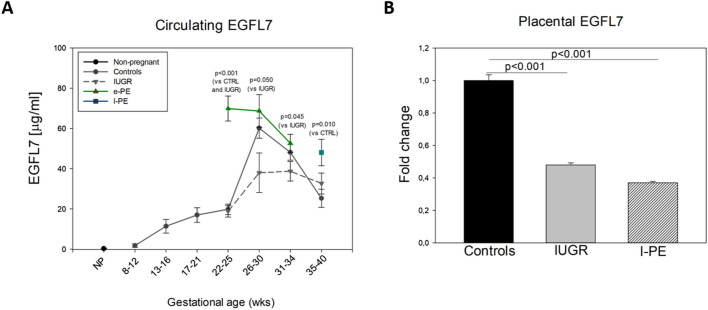
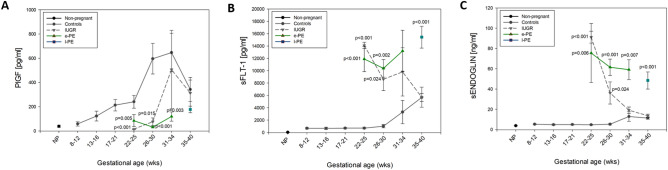
Isolated intrauterine growth restriction (IUGR) and preeclampsia (PE) share common placental pathogenesis. Differently from IUGR, PE is a systemic disorder which may also affect liver and brain. Early diagnosis of these conditions may optimize maternal and fetal management. Aim of this study was to assess whether Epidermal Growth Factor-Like domain 7 (EGFL7) dosage in maternal blood discriminates between isolated IUGR and PE. A total of 116 women were enrolled in this case-control study: 12 non-pregnant women, 34 healthy pregnant women, 34 women presenting with isolated IUGR and 36 presenting with PE. Levels of circulating EGFL7 and other known pro- and anti-angiogenic factors were measured by ELISA at different gestational ages (GA). Between 22-25 weeks of gestation, EGFL7 levels in early-onset PE (e-PE) plasma samples were significantly higher than those measured in controls or isolated IUGR samples (69.86 ± 6.17 vs. 19.8 ± 2.5 or 18.8 ± 2.8 µg/ml, respectively). Between 26-34 weeks, EGFL7 levels remained significantly higher in e-PE compared to IUGR. At term, circulating and placental EGFL7 levels were comparable between IUGR and late-onset PE (l-PE). In contrast, circulating levels of PlGF were decreased in both IUGR- and PE- complicated pregnancies, while levels of both sFLT-1 and sENDOGLIN were increased in both conditions. In conclusion, EGFL7 significantly discriminates between isolated IUGR and PE.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Resnik R. Intrauterine growth restriction. Obstet. Gynecol. 2002;99:490–496. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
