

Current Therapies for Neonatal Hypoxic-Ischaemic and Infection-Sensitised Hypoxic-Ischaemic Brain Damage
- PMID: 34504417
- PMCID: PMC8421799
- DOI: 10.3389/fnsyn.2021.709301
Current Therapies for Neonatal Hypoxic-Ischaemic and Infection-Sensitised Hypoxic-Ischaemic Brain Damage
Abstract
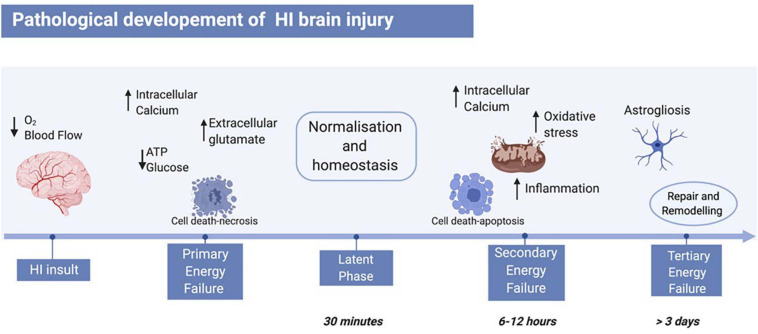
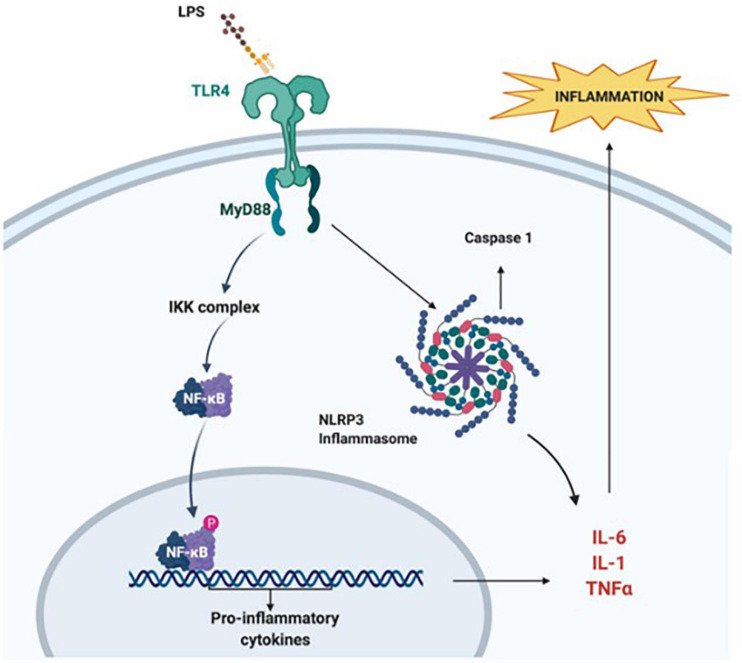
Neonatal hypoxic-ischaemic brain damage is a leading cause of child mortality and morbidity, including cerebral palsy, epilepsy, and cognitive disabilities. The majority of neonatal hypoxic-ischaemic cases arise as a result of impaired cerebral perfusion to the foetus attributed to uterine, placental, or umbilical cord compromise prior to or during delivery. Bacterial infection is a factor contributing to the damage and is recorded in more than half of preterm births. Exposure to infection exacerbates neuronal hypoxic-ischaemic damage thus leading to a phenomenon called infection-sensitised hypoxic-ischaemic brain injury. Models of neonatal hypoxia-ischaemia (HI) have been developed in different animals. Both human and animal studies show that the developmental stage and the severity of the HI insult affect the selective regional vulnerability of the brain to damage, as well as the subsequent clinical manifestations. Therapeutic hypothermia (TH) is the only clinically approved treatment for neonatal HI. However, the number of HI infants needed to treat with TH for one to be saved from death or disability at age of 18-22 months, is approximately 6-7, which highlights the need for additional or alternative treatments to replace TH or increase its efficiency. In this review we discuss the mechanisms of HI injury to the immature brain and the new experimental treatments studied for neonatal HI and infection-sensitised neonatal HI.
Keywords: hypoxia; infection; ischaemia; neonatal brain damage; neonatal encephalopathy.
Copyright © 2021 Tetorou, Sisa, Iqbal, Dhillon and Hristova.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources