

Ocular Immune-Related Adverse Events Associated With Immune Checkpoint Inhibitors in Lung Cancer
- PMID: 34504488
- PMCID: PMC8421677
- DOI: 10.3389/fimmu.2021.701951
Ocular Immune-Related Adverse Events Associated With Immune Checkpoint Inhibitors in Lung Cancer
Abstract
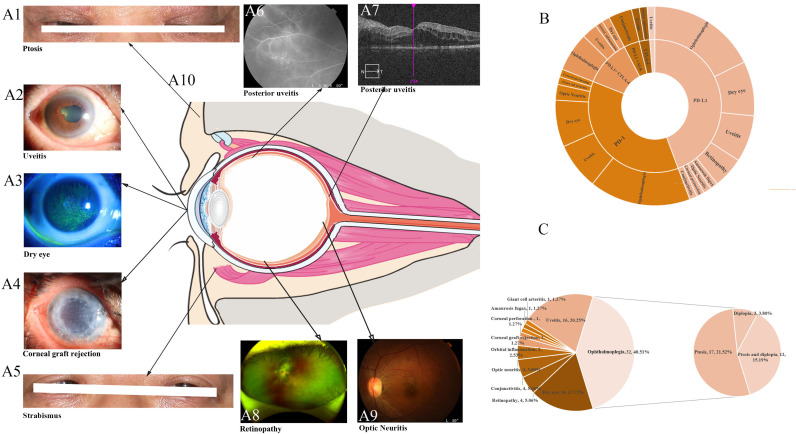
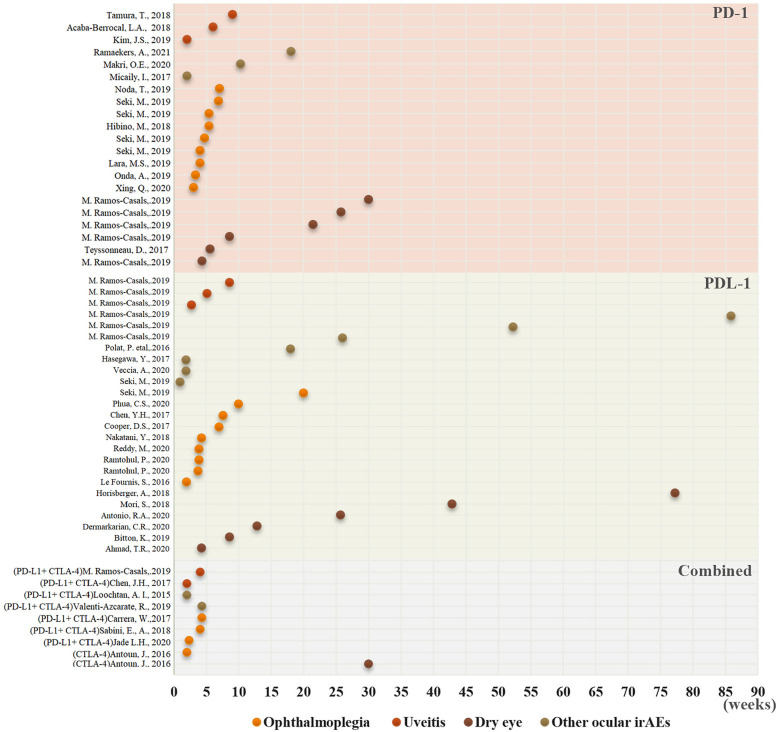
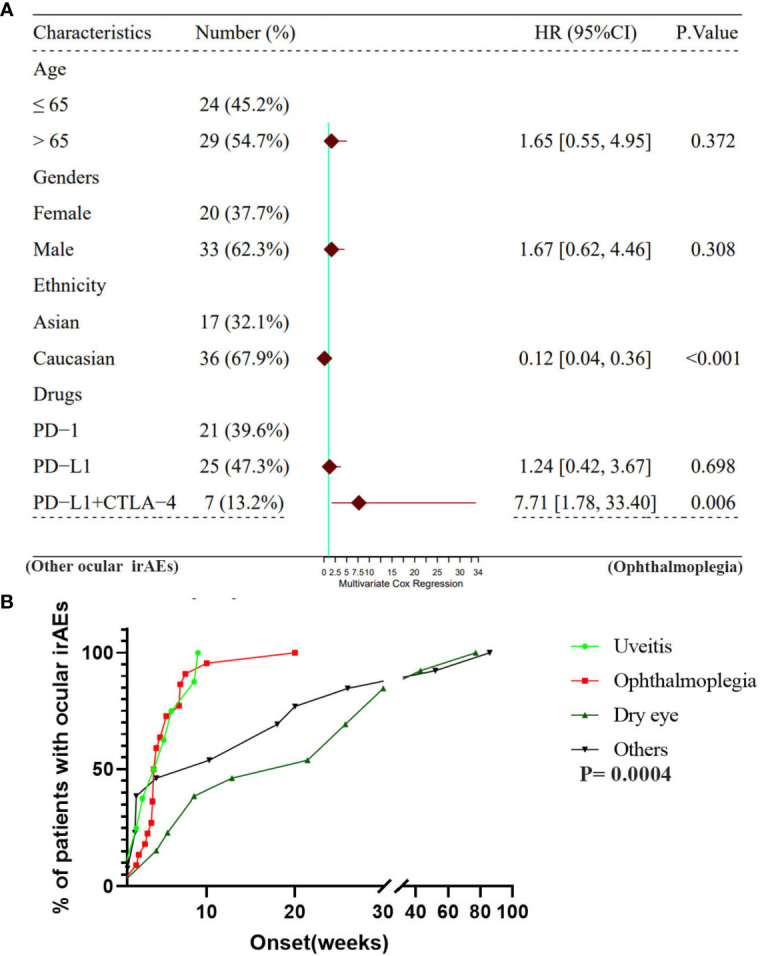
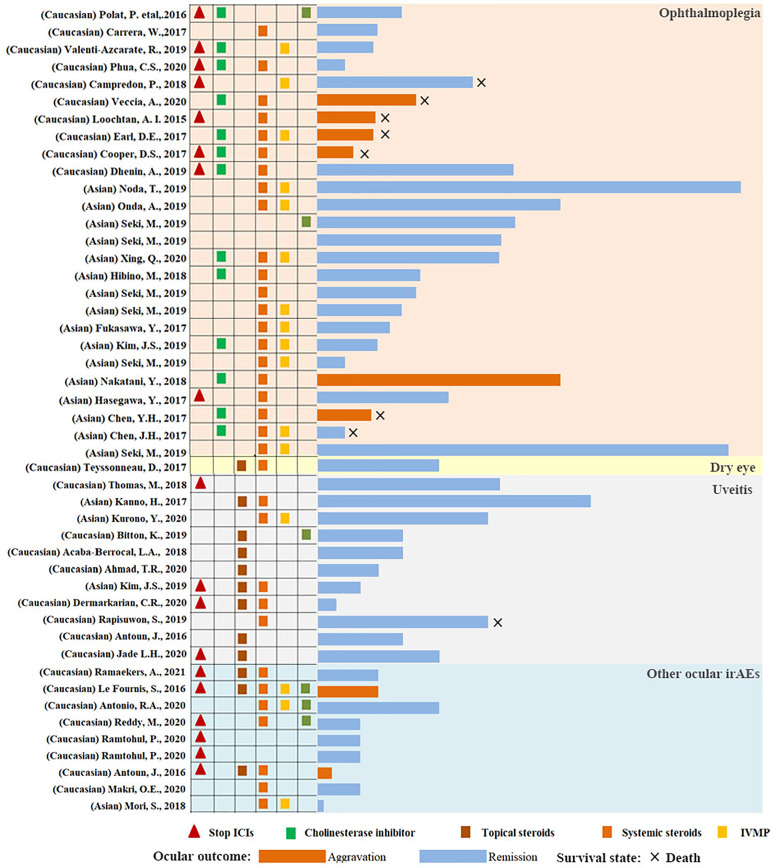
Immune checkpoint inhibitors (ICIs) are novel immunotherapy-based drugs that have become increasingly popular in the treatment of lung cancer. Researchers have recognized ocular immune-related adverse events (irAEs) secondary to ICIs because of their vision-threatening characteristics. However, they are incompletely characterized and no studies have reported the ICI-related ocular irAEs in lung cancer. Therefore, we aimed to comprehensively illustrate the clinical characteristics, contributory factors, diagnosis, and management of ICI-related ocular irAEs in lung cancer, based on previously reported 79 patients. Ophthalmoplegia (40.51%), uveitis (20.25%), and dry eye (17.72%) were the most common ICI-related ocular irAEs in lung cancer. Ptosis was the most common (36.71%) and the highest mortality (23.33%) of ophthalmoplegia. Patients in Asia and patients who underwent combination therapy with programmed cell death-1 and cytotoxic T-lymphocyte-associated antigen 4 inhibitors demonstrated significantly higher frequency of ophthalmoplegia than other ocular irAEs. Most ICI-related ophthalmoplegia and uveitis in lung cancer were observed in the first 10 weeks following the initiation of ICIs. Furthermore, the onset time of dry eye and other ocular irAEs was much longer. In addition, 92.31% of the patients with ocular irAEs other than ophthalmoplegia could be remised. In conclusion, ocular irAEs secondary to ICIs in lung cancer are non-negligible, particularly ophthalmoplegia. Ethnicity and the type of ICIs play important roles in the distribution of ocular irAEs. ICI-related ophthalmoplegia in lung cancer presented with early onset and worse prognosis features, thus necessitating further attention.
Keywords: dry eye; immune checkpoint inhibitors; lung cancer; ocular immune-related adverse events; ophthalmoplegia; uveitis.
Copyright © 2021 Zhou and Wei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical